Chapter: Human Nervous System and Sensory Organs : Spinal Cord and Spinal Nerves
Spinal Cord Syndromes
Spinal Cord Syndromes
The
anatomy of the spinal cord causes very specific patterns of functional
deficiencies after injury; depending on the site of lesion, different pathways
and therefore different functions are lost.
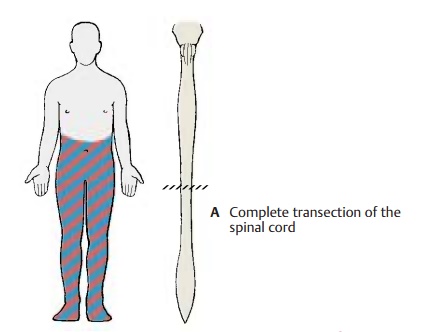
Complete transection (A) cuts off all de-scending motor pathways, causing completeparalysis below the injured
level. At thesame time, it interrupts all ascending path-ways, causing a
complete loss of all sensa-tions. If
the lesion is above the sacral spinalcord, it results in the loss of voluntary
con-trol over urination and defecation. If the le-sion lies above the lumbar
enlargement, both lower limbs are paralyzed (paraplegia), and if it lies above the cervical enlargement, both
upper limbs are also paralyzed (tet-
raplegia).
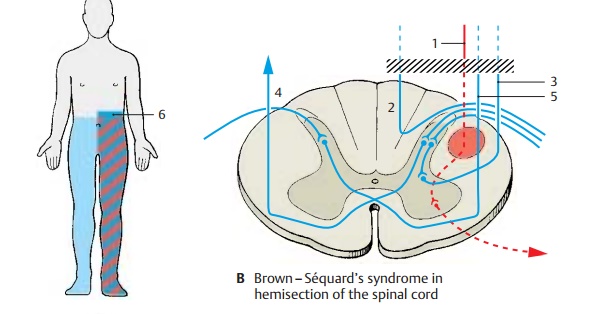
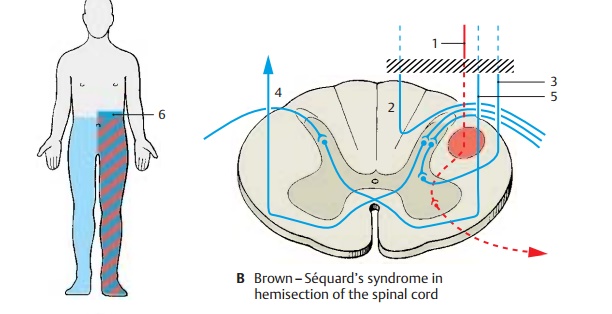
Hemisection of the spinal cord (B) results inthe Brown – Séquard’s syndrome. For example, hemisection on the left
interrupts the lateral and anterior corticospinal tracts (B1) and results in left-sided paralysis.
Transec-tion of the vasomotor pathway causes ipsi-lateral vasomotor paralysis.
Transection of the posterior funiculi (B2)
and the cerebel-lar lateral funiculi (B3)
leads to severely im-paired deep
sensibility (posture sensation).On the same side as the lesion, there is
also hyperesthesia (touch is
perceived as pain).This is thought to be caused by a loss of epicritic
sensibility (posterior funiculi) with retention of the protopathic sensibility
(crossing pathways of the anterior corti-cospinal tract ascend contralaterally)
(B4). Finally, there is dissociated anesthesia on the intact
right side from the lesion downward; while touch sensation is hardly impaired,
pain and temperature sensations are lost (ipsilateral interruption of the
crossing pathway of the anterior corticospinal tract) (B5). The anesthetic zone (B6)
above the transection on the affected side is attributed to destruction of the
posterior root entrance zone at the level of the spinal cord lesion.
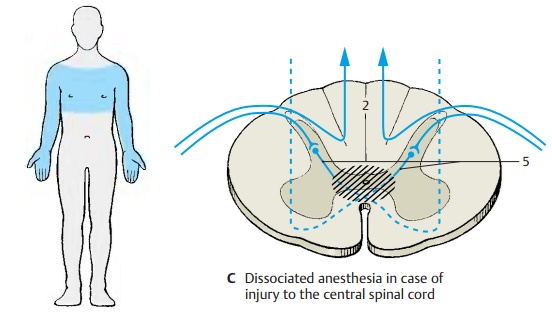
Central injury (C) to the gray substance ofthe spinal cord also causes dissociated anes-thesia at the
corresponding levels. Theepicritic sensibility transmitted via the ipsi-lateral
posterior funiculi (C2) is retained.
However, pain and temperature sensations are lost (analgesia and thermoanesthesia),
be-cause their fibers, which cross through the white commissure, are
interrupted (C5).
Related Topics