Chapter: Human Nervous System and Sensory Organs : Spinal Cord and Spinal Nerves
Segmental Innervation - Spinal Cord
Segmental Innervation
The
vertebrate body, with the exception of the head, is originally subdivided into segments or metameres. The vertebrae, ribs, andintercostal muscles can be
regarded as rem-nants of such a segmentation in humans. Metamerism concerns
only tissues of the mesoderm (myotomes,
sclerotomes) but not derivatives of
the ectoderm. Thus, there are no spinal cord segments, only the levels at which
the individual spinal roots enter and emerge. However, the spinal fibers join
to form the spinal nerves as they emerge through the metameric intervertebral
foramina, thus creating an apparent
second-ary segmentation. The sensory fibers of thespinal nerves supply
stripe-shaped zones of the skin, called dermatomes
in analogy to myotomes and sclerotomes. This, too, is a secondary segmentation
and reflects the in-nervation of each dermatome by a single posterior root
(segmental innervation).
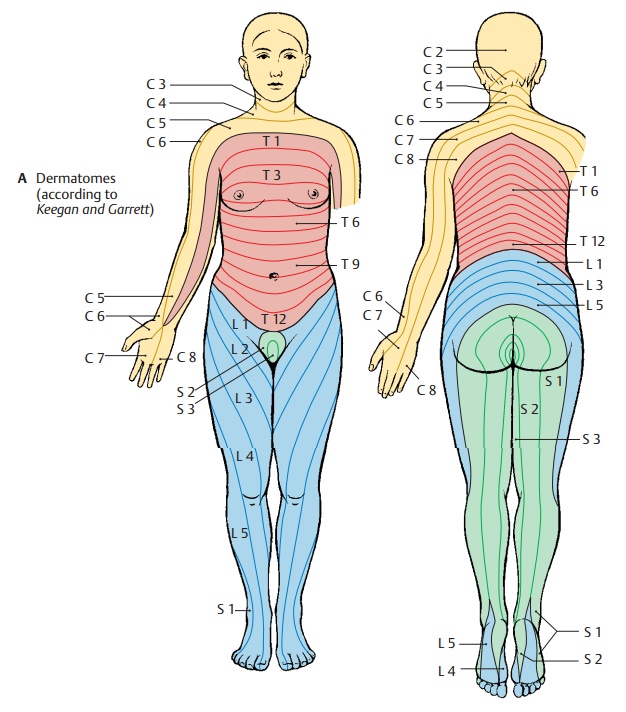
Clinical Note: The dermatomes play an im-portant
role in the diagnosis and localization
ofspinal cord injuries. Loss of sensibility in certaindermatomes indicates
a specific level of injury in the spinal cord. Simplified reference points are
the line through the nipples, regarded as the boundary between T4 and T5, and
the groin, re-garded as the boundary between L1 and L2. The first cervical
spinal nerve has no sensory repre-sentation on the body surface, for the spinal
gan-glion of its posterior root is absent or rudimen-tary.
There
are slightly different segmental boundaries for various modalities, such as
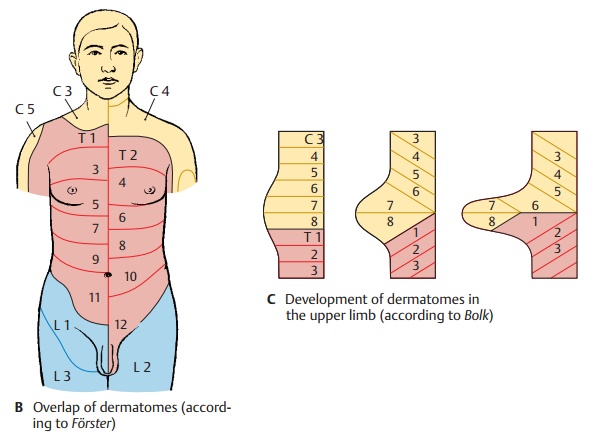
touch and pain, and for sweating and piloerection. The diagram (A) was designed according to the decrease in sensibility (hy-poesthesia) resulting from disk
prolapse; itshows how the dermatomes extending around the trunk become
elongated in the limbs. They may even lose their continuity with the midline
(C7, L5). They become translocated to the distal limb areas during embryonic
development when the limbs are budding (C).
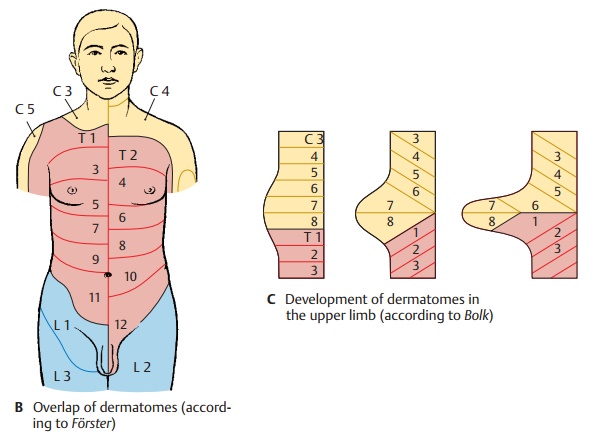
The
dermatomes overlap like roof tiles, as il-lustrated by the shift in boundaries
that have been determined according to the ex-panded areas in case of posterior root pain (hypersensitivity to
pain, hyperalgesia) (B). The loss of a single posterior root
cannot be demonstrated for touch sensation, since the corresponding dermatome
is also supplied by the neighboring posterior roots. The der-matomes for pain
and temperature sensa-tion are narrower, and the loss of a posterior root can
still be demonstrated when these modalities are tested.
Related Topics