Chapter: Basic & Clinical Pharmacology : Adrenoceptor Antagonist Drugs
Specific Agents
SPECIFIC AGENTS (SEE TABLE 10–2)
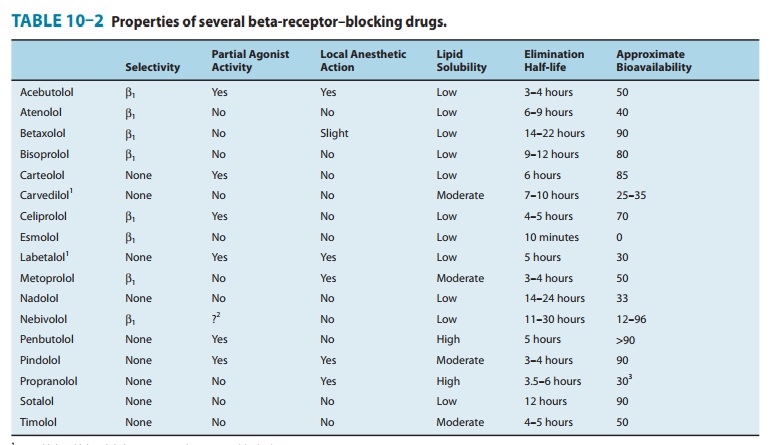
Propranolol is the prototypicalβ-blocking drug. As noted before,it has low and
dose-dependent bioavailability. A long-acting form of propranolol is available;
prolonged absorption of the drug may occur over a 24-hour period. The drug has
negligible effects at α and muscarinic receptors; however, it may
block some serotonin receptors in the brain, though the clinical significance
is unclear. It has no detectable partial agonist action at β receptors.
Metoprolol, atenolol, and several other
drugs (Table 10–2) aremembers of the β1-selective group. These agents may be safer in
patients who experience bronchoconstriction in response to pro-pranolol. Since
their β1 selectivity is rather modest, they should be used with great
caution, if at all, in patients with a history of asthma. However, in selected
patients with COPD the benefits may exceed the risks, eg, in patients with
myocardial infarction. Beta1-selective antagonists may be preferable
in patients with dia-betes or peripheral vascular disease when therapy with a β blocker is required,
since β2 receptors are probably important in liver (recovery from
hypoglycemia) and blood vessels (vasodilation).
Nebivolol is the most highly selectiveβ1-adrenergic
receptorblocker, though some of its metabolites do not have this level of
specificity. Nebivolol has the additional quality of eliciting vasodi-lation.
This is due to an action of the drug on endothelial nitricoxide production.
Nebivolol may increase insulin sensitivity and does not adversely affect lipid
profile.
Nadolol is noteworthy for its very long duration of
action; itsspectrum of action is similar to that of timolol. Timolol is a non-selective agent with
no local anesthetic activity. It has excellent ocular hypotensive effects when
administered topically in the eye. Levobunolol
(nonselective) and betaxolol (β1-selective) are
alsoused for topical ophthalmic application in glaucoma; the latter drug may be
less likely to induce bronchoconstriction than non-selective antagonists. Carteolol is a nonselective β-receptor antagonist.
Pindolol, acebutolol, carteolol, bopindolol,* oxprenolol,* celiprolol,*and penbutolol are of interest because
they have par-tial β-agonist
activity. They are effective in the major cardiovascu-lar applications of the β-blocking group
(hypertension and angina). Although these partial agonists may be less likely
to cause bradycardia and abnormalities in plasma lipids than are antago-nists,
the overall clinical significance of intrinsic sympathomimetic activity remains
uncertain. Pindolol, perhaps as a result of actions on serotonin signaling, may
potentiate the action of traditional antidepressant medications. Celiprolol is
a β1-selective antagonist with a modest capacity to activate β2 receptors.
There
is limited evidence suggesting that celiprolol may have less adverse
bronchoconstrictor effect in asthma and may even promote bronchodilation.
Acebutolol is also a β1-selective antagonist.
Labetalol is a reversible adrenoceptor antagonist
available as aracemic mixture of two pairs of chiral isomers (the molecule has
two centers of asymmetry). The (S,S)-
and (R,S)-isomers are nearly
inactive, the (S,R)-isomer is a
potent α
blocker, and the (R,R)-isomer is a
potent β
blocker. Labetalol’s affinity for α receptors is less than that of phentolamine,
but labetalol is α1-selective. Its β-blocking potency is somewhat lower than that
of propranolol.Hypotension induced by labetalol is accompanied by less
tachy-cardia than occurs with phentolamine and similar α blockers.
Carvedilol, medroxalol,*and bucindolol*are nonselectiveβ-receptor antagonists with some capacity to
block α1-adrenergicreceptors. Carvedilol antagonizes the actions of
catecholamines more potently at β receptors than at α1 receptors. The drug has a half-life of 6–8
hours. It is extensively metabolized in the liver, and stereoselective
metabolism of its two isomers is observed. Since metabolism of (R)-carvedilol is influenced by
polymorphisms in CYP2D6 activity and by drugs that inhibit this enzyme’s
activity (such as quinidine and fluoxetine,), drug interac-tions may occur.
Carvedilol also appears to attenuate oxygen free radical–initiated lipid
peroxidation and to inhibit vascular smooth muscle mitogenesis independently of
adrenoceptor blockade. These effects may contribute to the clinical benefits of
the drug in chronic heart failure .
Esmolol is an ultra-short–actingβ1-selective
adrenoceptorantagonist. The structure of esmolol contains an ester linkage;
esterases in red blood cells rapidly metabolize esmolol to a metab-olite that
has a low affinity for β receptors. Consequently, esmolol has a short
half-life (about 10 minutes). Therefore, during con-tinuous infusions of
esmolol, steady-state concentrations are achieved quickly, and the therapeutic
actions of the drug are ter-minated rapidly when its infusion is discontinued.
Esmolol may be safer to use than longer-acting antagonists in critically ill
patients who require a β-adrenoceptor antagonist. Esmolol is use-ful
in controlling supraventricular arrhythmias, arrhythmias asso-ciated with
thyrotoxicosis, perioperative hypertension, and myocardial ischemia in acutely
ill patients.
Butoxamine is a research drug selective forβ2receptors.Selective β2-blocking drugs have
not been actively sought because there is no obvious clinical application for
them; none is available for clinical use.
Related Topics