Chapter: Basic & Clinical Pharmacology : Adrenoceptor Antagonist Drugs
Clinical Pharmacology of the Alpha Receptor Blocking Drugs
CLINICAL PHARMACOLOGY OF THE
ALPHA RECEPTOR BLOCKING DRUGS
Pheochromocytoma
Pheochromocytoma
is a tumor of the adrenal medulla or sympa-thetic ganglion cells. The tumor
secretes catecholamines, espe-cially norepinephrine and epinephrine. The
patient in the case study at the beginning had a left adrenal pheochro-mocytoma
that was identified by imaging. In addition, she had elevated plasma and
urinary norepinephrine, epinephrine, and their metabolites, normetanephrine and
metanephrine.
The
diagnosis of pheochromocytoma is confirmed on the basis of elevated plasma or
urinary levels of catecholamines, metaneph-rine, and normetanephrine . Once
diagnosed bio-chemically, techniques to localize a pheochromocytoma include
computed tomography and magnetic resonance imaging scans and scanning with
radiomarkers such as 131I-meta-iodobenzylguanidine (MIBG), a
norepinephrine transporter substrate that is taken up by tumor cells.
The
major clinical use of phenoxybenzamine is in the manage-ment of
pheochromocytoma. Patients have many symptoms and signs of catecholamine
excess, including intermittent or sustained hypertension, headaches,
palpitations, and increased sweating.
Release
of stored catecholamines from pheochromocytomas may occur in response to
physical pressure, chemical stimulation, or spontaneously. When it occurs
during operative manipulation of pheochromocytoma, the resulting hypertension
may be con-trolled with α-receptor blockade or nitroprusside.
Nitroprusside is preferred because its effects can be more readily titrated and
it has a shorter duration of action.
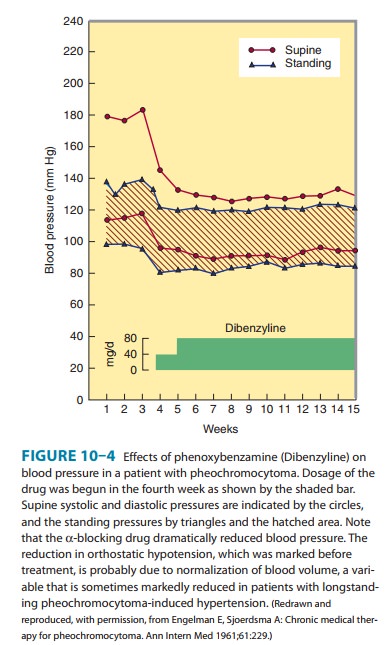
Alpha-receptor antagonists are most useful in the preoperative management of patients with pheochromocytoma (Figure 10–4). Administration of phenoxybenzamine in the preoperative period helps to control hypertension and tends to reverse chronic changes resulting from excessive catecholamine secretion such as plasma volume contraction, if present. Furthermore, the patient’s opera-tive course may be simplified. Oral doses of 10 mg/d can be increased at intervals of several days until hypertension is con-trolled. Some physicians give phenoxybenzamine to patients with pheochromocytoma for 1–3 weeks before surgery. Other surgeons prefer to operate on patients in the absence of treatment with phenoxybenzamine, counting on modern anesthetic techniques to control blood pressure and heart rate during surgery. Phenoxybenzamine can be very useful in the chronic treatment of inoperable or metastatic pheochromocytoma. Although there is less experience with alternative drugs, hypertension in patients with pheochromocytoma may also respond to reversible α1-selective antagonists or to conventional calcium channel antago-nists. Beta-receptor antagonists may be required after α-receptor blockade has been instituted to reverse the cardiac effects of exces-sive catecholamines. Beta antagonists should not be used prior to establishing effective α-receptor blockade, since unopposed β-receptor blockade could theoretically cause blood pressure eleva-tion from increased vasoconstriction.
Pheochromocytoma
is sometimes treated with metyrosine
(α-methyltyrosine),
the α-methyl
analog of tyrosine. This agent is a competitive inhibitor of tyrosine
hydroxylase, the rate-limiting step in the synthesis of dopamine,
norepinephrine, and epineph-rine (see Figure 6–5). Metyrosine is especially
useful in symptom-atic patients with inoperable or metastatic pheochromocytoma.
Because it has access to the central nervous system, metyrosine can cause
extrapyramidal effects due to reduced dopamine levels.
Hypertensive Emergencies
The
α-adrenoceptor
antagonist drugs have limited application in the management of hypertensive
emergencies, but labetalol has been used in this setting . In theory, α-adrenoceptor
antagonists are most useful when increased blood pressure reflects excess
circulating concentrations of α agonists, eg, in pheochro-mocytoma,
overdosage of sympathomimetic drugs, or clonidine withdrawal. However, other
drugs are generally preferable, since considerable experience is necessary to
use α-adrenoceptor
antag-onist drugs safely in these settings.
Chronic Hypertension
Members
of the prazosin family of α1-selective antagonists are effica-cious drugs
in the treatment of mild to moderate systemic hyperten-sion . They are
generally well tolerated, but they are not usually recommended as monotherapy
for hypertension because other classes of antihypertensives are more effective
in preventing heart failure. Their major adverse effect is orthostatic
hypotension, which may be severe after the first few doses but is otherwise
uncom-mon. Nonselective αantagonists are not used in primary systemic
hypertension. Prazosin and related drugs may also be associated with dizziness.
Orthostatic changes in blood pressure should be checked routinely in any
patient being treated for hypertension.
It
is interesting that the use of α-adrenoceptor antagonists such as prazosin has
been found to be associated with either no changes in plasma lipids or
increased concentrations of high-density lipo-proteins (HDL), which could be a
favorable alteration. The mechanism for this effect is not known.
Peripheral Vascular Disease
Alpha-receptor–blocking
drugs do not seem to be effective in the treatment of peripheral vascular
occlusive disease characterized by morphologic changes that limit flow in the
vessels. Occasionally, individuals with Raynaud’s phenomenon and other
conditions involving excessive reversible vasospasm in the peripheral
circula-tion do benefit from prazosin or phenoxybenzamine, although calcium
channel blockers may be preferable for most patients.
Urinary Obstruction
Benign
prostatic hyperplasia is common in elderly men. Various surgical treatments are
effective in relieving the urinary symptoms of BPH; however, drug therapy is
efficacious in many patients. The mechanism of action in improving urine flow
involves partial reversal of smooth muscle contraction in the enlarged prostate
and in the bladder base. It has been suggested that some α1-receptor antagonists
may have additional effects on cells in the prostate that help improve
symptoms.
Prazosin,
doxazosin, and terazosin are all efficacious in patients with BPH. These drugs
are particularly useful in patients who also have hypertension. Considerable
interest has focused on which α1-receptor subtype is most important for smooth
muscle contrac-tion in the prostate: subtype-selectiveα1A-receptor antagonists
may have improved efficacy and safety in treating this disease. As indi-cated
above, tamsulosin is also efficacious in BPH and has rela-tively minor effects
on blood pressure at a low dose. This drug may be preferred in patients who
have experienced orthostatic hypoten-sion with other α1-receptor antagonists.
Erectile Dysfunction
A
combination of phentolamine with the nonspecific smooth muscle relaxant
papaverine, when injected directly into the penis, may cause erections in men
with sexual dysfunction. Long-term administration may result in fibrotic
reactions. Systemic absorption may lead to orthostatic hypotension; priapism
may require direct treatment with anα-adrenoceptor agonist such as phenylephrine.
Alternative therapies for erectile dysfunction include prostaglan-dins ,
sildenafil and other cGMP phosphodi-esterase inhibitors , and apomorphine.
Applications of Alpha2 Antagonists
Alpha2
antagonists have relatively little clinical usefulness. They have limited
benefit in male erectile dysfunction. There has been experimental interest in
the development of highly selective antag-onists for treatment of type 2
diabetes (α2 receptors inhibit insulin secretion), and for treatment of
psychiatric depression. It is likely that better understanding of the subtypes
of α2 receptors will lead to development of clinically useful
subtype-selective new drugs.
Related Topics