Chapter: Medical Microbiology: An Introduction to Infectious Diseases: Influenza, Respiratory Syncytial Virus, Adenovirus, and Other Respiratory Viruses
Respiratory Syncytial Virus Disease : Clinical Aspects
RESPIRATORY SYNCYTIAL VIRUS DISEASE : CLINICAL ASPECTS
MANIFESTATIONS
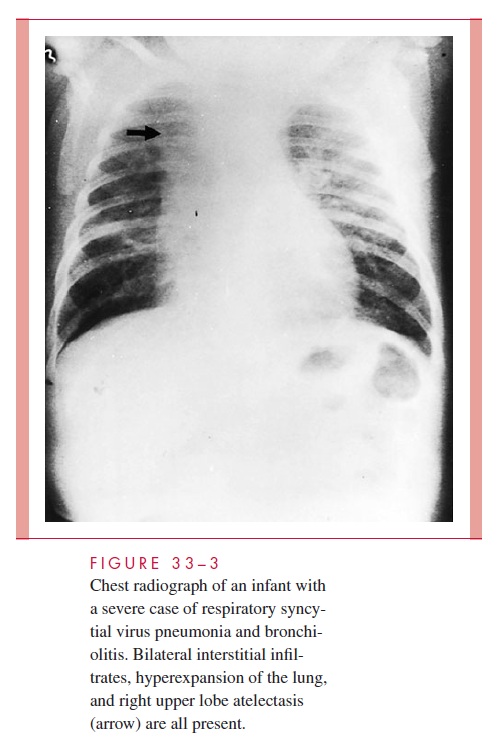
The usual incubation period is 2 to 4 days, followed by the onset of rhinitis; severity of illness progresses to a peak within 1 to 3 days. In infants, this peak usually takes the form of bronchiolitis and pneumonitis, with cough, wheezing, and respiratory distress. Clinical findings include hyperexpansion of the lungs, hypoxemia (low oxygenation of blood), and hypercapnia (carbon dioxide retention). Interstitial infiltrates, often with areas of pulmonary collapse, may be seen on chest radiography (Fig 33–3). Fever is variable. The duration of acute illness is often 10 to 14 days.
The fatality rate among hospitalized infected infants is estimated to be 0.5 to 1%; however, this rises to 15% or greater in children receiving cancer chemotherapy, infants with congenital heart disease, and those with severe immunodeficiency. Infants with underlying chronic lung disease are also at high risk. Causes of death include respira-tory failure, right-sided heart failure (cor pulmonale), and bacterial superinfection. Death has sometimes resulted from unnecessary procedures in patients in whom RSV infection was not considered. Bronchoscopy, lung biopsy, or overly aggressive therapy with corticosteroids and bronchodilators for presumed asthma can all pose a danger to such patients.
Older infants, children, and adults are also readily infected. The clinical illnesses in these groups are usually milder and include croup, tracheobronchitis, and upper respira-tory infection (URI); however, elderly persons can experience severe morbidity. RSV can also cause acute flare-ups of chronic bronchitis and trigger acute wheezing episodes in asthmatic children.
DIAGNOSIS
Rapid diagnosis of RSV infection can be made by immunofluorescence or immunoenzyme detection of viral antigen. The virus can also be isolated from the respiratory tract by prompt inoculation of specimens into cell cultures. Syncytial cytopathic effects develop over 2 to 7 days. Serodiagnosis may also be used but requires acute and convales-cent sera and is less sensitive than antigen detection methods or culture.
TREATMENT AND PREVENTION
Treatment is directed primarily at the underlying pathophysiology and includes adequate oxygenation, ventilatory support when necessary, and close observation for complications such as bacterial superinfection and right-sided heart failure. Some studies suggest that ribavirin aerosol treatment may be effective in selected circumstances.
No vaccine is currently available. Attenuated live virus vaccines and immune globulin containing high antibody titers to RSV are also under active investigation; a high-titered monoclonal antibody against F protein has been used for prophylaxis in high-risk infants (those born prematurely or with chronic lung disease). This method requires monthly in-jections during the RSV season (usually 5 months) and is extremely expensive.
Related Topics