Chapter: Basic & Clinical Pharmacology : Diuretic Agents
Proximal Tubule - Renal Tubule Transport Mechanisms
RENAL TUBULE
TRANSPORT MECHANISMS
PROXIMAL TUBULE
Sodium
bicarbonate (NaHCO3), sodium chloride (NaCl), glu-cose, amino acids,
and other organic solutes are reabsorbed via specific transport systems in the
early proximal tubule (proximal convoluted tubule, PCT). Potassium ions (K+) are reabsorbed via
the paracellular pathway. Water is reabsorbed passively, maintain-ing the
osmolality of proximal tubular fluid at a nearly constant level. As tubule
fluid is processed along the length of the proximal tubule, the luminal
concentrations of these solutes decrease rela-tive to the concentration of
inulin, an experimental marker that is filtered but neither secreted nor
absorbed by renal tubules. Approximately 66% of filtered sodium ions (Na+), 85% of the NaHCO3,
65% of the K+, 60% of the water, and virtually all of the filtered glucose
and amino acids are reabsorbed in the proxi-mal tubule.
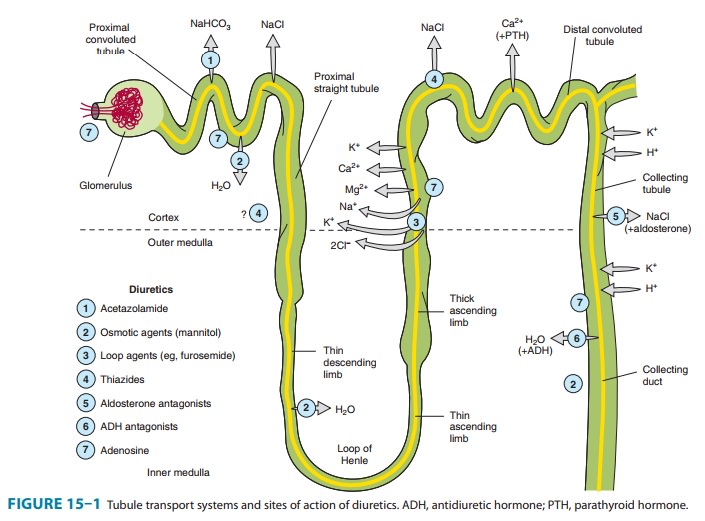
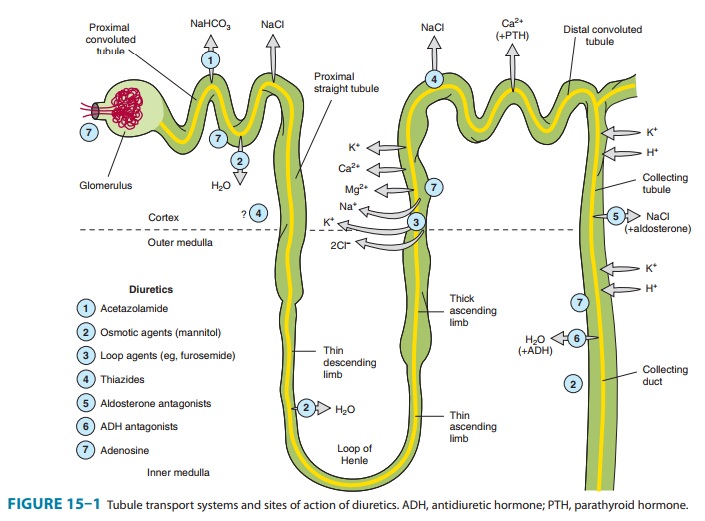
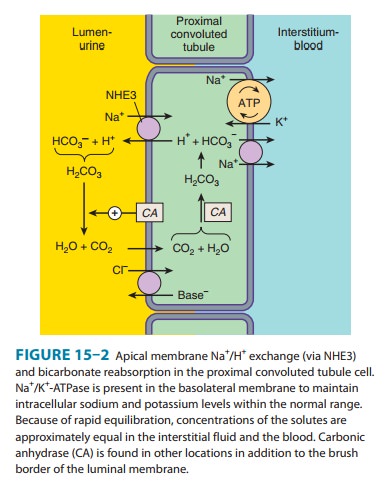
Of the various solutes reabsorbed in the proximal tubule, the most relevant to diuretic action are NaHCO3 and NaCl. Of the currently available diuretics, only one group (carbonic anhydrase inhibitors, which block NaHCO3 reabsorption) acts predomi-nantly in the PCT. In view of the large quantity of NaCl absorbed in this segment, a drug that specifically blocked proximal tubular absorption of NaCl could be a particularly powerful diuretic. Adenosine receptor antagonists, which are currently under intense clinical investigation, act mainly in the PCT and appear to induce a NaCl, rather than a NaHCO3 diuresis. Sodium bicarbonate reabsorption by the PCT is initiated by the action of a Na+/H+ exchanger (NHE3) located in the luminal membrane of the proximal tubule epithelial cell (Figure 15–2). This transport sys-tem allows Na+ to enter the cell from the tubular lumen in exchange for a proton (H+) from inside the cell. As in all portions of the nephron, Na+/K+-ATPase in the basolateral membrane pumps the reabsorbed Na+ into the interstitium so as to maintain a low intracellular Na+ concentration. The H+ secreted into the lumen combines with bicarbonate (HCO3−) to form H2CO3 (car-bonic acid), which is rapidly dehydrated to CO2 and H2O by carbonic anhydrase. Carbon dioxide produced by dehydration of H2CO3 enters the proximal tubule cell by simple diffusion where it is then rehydrated back to H2CO3, also facilitated by intracel-lular carbonic anhydrase. After dissociation of H2CO3, the H+ is available for transport by the Na+/H+ exchanger, and the HCO3− is transported out of the cell by a basolateral membrane trans-porter (Figure 15–2). Bicarbonate reabsorption by the proximal tubule is thus dependent on carbonic anhydrase activity. This enzyme can be inhibited by acetazolamide and other carbonic anhydrase inhibitors.
Adenosine,
which is released as a result of hypoxia and ATP consumption, is a molecule
with four different receptors and com-plex effects on Na+ transport in several
segments of the nephron. Although it reduces glomerular filtration rate (GFR)
to decrease energy consumption by the kidney, adenosine actually increases
proximal reabsorption of Na+ via stimulation of NHE3 activity. A new class of drugs, the
adenosine A1-receptor antagonists, have recently been found to
significantly blunt both proximal tubule NHE3 activity and collecting duct NaCl
reabsorption, and to have potent vasomotor effects in the renal
microvasculature (, under Autacoids, Pharmacology of Diuretic Agents, and under
Heart Failure).
Because
HCO3− and organic solutes have been largely removed from
the tubular fluid in the late proximal tubule, the residual luminal fluid
contains predominantly NaCl. Under these condi-tions, Na+ reabsorption
continues, but the H + secreted by the Na+/H+ exchanger can no
longer bind to HCO3−. Free H+ causes luminal pH to
fall, activating a poorly defined Cl−/base exchanger (Figure 15–2).
The net effect of parallel Na+/H+ exchange and Cl−/base exchange is NaCl reabsorption.
As yet, there are no diuretic agents that are known to act on this conjoint
process.
Water
is reabsorbed in the PCT in response to osmotic forces, so luminal fluid
osmolality remains nearly constant along its length, and an impermeant solute
like inulin rises in concentra-tion as water is reabsorbed. If large amounts of
an impermeant solute such as mannitol (an osmotic diuretic) are present in the
tubular fluid, water reabsorption causes the concentration of the solute to
rise, so that as salt concentrations become diminished further, water reabsorption
is prevented.
Organic
acid secretory systems are located in the middle third of the straight part of
the proximal tubule (S2 segment). These systems secrete a variety of
organic acids (uric acid, nonsteroidal anti-inflam-matory drugs [NSAIDs],
diuretics, antibiotics, etc) into the luminal fluid from the blood. These
systems thus help deliver diuretics to the luminal side of the tubule, where
most of them act. Organic base secretory systems (creatinine, choline, etc) are
also present, in the early (S1) and middle (S2) segments
of the proximal tubule.
Related Topics