Chapter: Modern Medical Toxicology: Organic Poisons (Toxins): Venomous Bites and Stings
Order Scorpionida - Venomous Arachnids

VENOMOUS ARACHNIDS
Arachnids
differ from insects mainly in the number of legs they possess: eight instead of
six. There are two important orders from the toxicological point of view:
Scorpionida and Aranea, both belonging to subphylum Chelicerata.
ORDER SCORPIONIDA
The members of this order comprise scorpions, which are capable of inflicting severe, and sometimes fatal stings. There are at least 650 different types of scorpions divided into 6 families. Most species are nocturnal, and seek areas that are cool and moist.
Anatomy
·
The scorpion has a cephalothorax
(fused head and chest), an abdomen, and a six segmented tail which terminates
in a bulbous enlargement called telson. The telson contains the stinger and
venom apparatus. In addition, the scorpion also has two claws (chelae or
pedipalps) which help to grasp its prey. Scorpions differ in colour from straw
yellow or light brown, to black.
·
The commonest species seen in India is Mesobuthus tamulus (red scorpion) (Fig 12.39). It grows up to 3 inches in length. Larger scorpions are
found in the outdoors (Palamnaeusspecies)
which grow up to 7 inches (Fig 12.40).


·
As a general rule, scorpions with thick and powerful claws
are less toxic, while those with slender claws are more toxic.
·
Scorpions sting; they do not bite.
Venom
Components of scorpion venom are complex and species-specific, those of the family Buthidae being the most potent. The main toxins include phospholipase, acetylcholinesterase, hyaluronidase, serotonin, and neurotoxins. The venom of Buthus species of India contains phospholipase A, which causesgastrointestinal and pulmonary haemorrhages, and dissemi-nated intravascular coagulation.
Mode of Action
·
Most scorpion venoms affect sodium
channels with prolon-gation of action potentials, as well as spontaneous
depo-larisation of nerves of both adrenergic and parasympathetic nervous
systems. Thus, both adrenergic and cholinergic symptoms occur.
·
Hyperkalaemia, hyperglycaemia (with
reduction in insulin secretion), and increased secretion of renin and
aldosterone are characteristic of stings by Mesobuthus
tamulus.
Clinical Features
A. Local
1. Rapidly developing, excruciating local pain,
swelling, redness, and regional lymphadenopathy.
B. Systemic
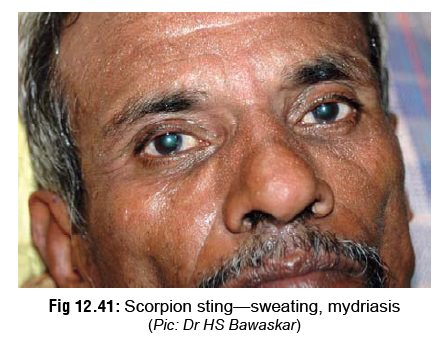
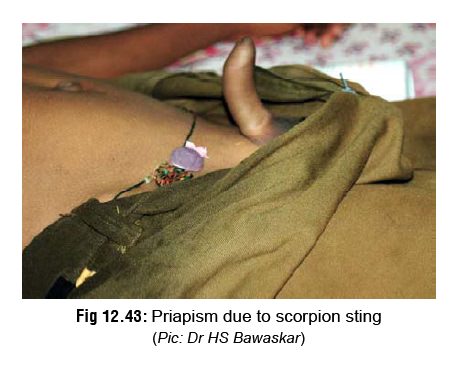
1. Signs of autonomic stimulation occur,
comprising mydri-asis, profuse sweating (Fig
12.41), urticaria, excessive salivation (Fig 12.42), vomiting, parasternal lift, priapism (Fig 12.43), hypertension,
brady-/tachyarrhythmias, and ventricular premature contractions.

2. Pulmonary oedema may develop within 2 to 3 hours leading to death.
3. Intracerebral haemorrhage
resulting in hemiparesis, from a scorpion sting, has been reported. Convulsions
may occur.
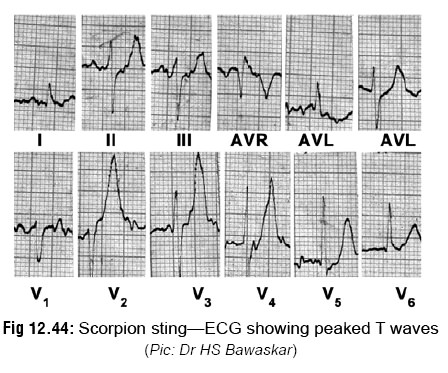
4. ECG changes: Early changes
suggestive of envenomation include peaked T waves in leads V2 to V6
( Fig 12.44), Q waves, ST-segment
elevation in leads I and AVL, and left anterior hemiblock.
5.Hyperglycaemia is common with most
species. Acute pancreatitis has been reported with some species.
6.
Allergic reactions, including anaphylaxis has occurred.
7.Palamnaeus species causes local
pain, paraesthesias, mild autonomic nervous system excitation, pulmonary
infiltra-tion, eosinophilia, salivation, nausea, sweating, and mild
hypotension.
8. Children under the age of 10 are
more likely to develop toxicity from most scorpion stings
than older victims. Effects are most severe in infants and toddlers.
Treatment
Most victims (without hypertension or cardiac disease) and children over the age of 5 can usually be handled at home with local application of ice and other supportive measures for pain relief. Patients with cardiac problems/hypertension, elderly victims, and children under the age of 5 should be referred to a hospital for evaluation.
During transport to hospital
·
Immobilise the affected extremity.
Do NOT apply tourniquet (Fig 12.45).

·
Local application of ice is beneficial in relieving pain.
·
Prolonged cryotherapy is however
contraindicated.
·
A negative-pressure suction device
may be used, if available, to extract venom at approximately 1 atm of negative
pressure (it is doubtful whether this really works). Do not incise prior
to suction.
On arrival at hospital
·
Admit all patients with systemic
manifestations (hyper-tension, hypovolaemia, pulmonary oedema) to intensive
care unit under close electrocardiographic, echocar-diographic, and if
necessary, invasive haemodynamic monitoring.
·
Patients with respiratory failure or
with CNS distur-bances should be mechanically ventilated; administer oxygen to
all serious cases.
·
Pain may be controlled by
paracetamol or morphine tablets.
·
Mild to moderate allergic reactions
may be treated with antihistamines, with or without inhaled beta agonists,
corticosteroids, or adrenaline. Treatment of severe anaphylaxis must include
oxygen supplementation, aggressive airway management, adrenaline, ECG
monitoring, and IV fluids.
·
Correct fluid and acid-base
imbalance. However, avoid infusing large amounts of fluids due to the risk of
pulmonary oedema. The pulmonary artery wedge pres-sure should be kept
relatively low while maintaining adequate cardiac output, blood pressure, and
urine output.
·
Some investigators claim prazocin
hydrochloride acts as an antagonist to scorpion venom, and is also
cardio-protective. The recommended dose is 500 micrograms every 4 to 6 hours
for adults, and 250 micrograms every 4 to 6 hours for children.
·
Hypertension (>160/110 mmHg) is
conventionally managed with nifedipine at a dose of 10 to 20 mg (adults) or 0.3
mg/kg (children) every 4 to 6 hours.
· Bawaskar & Bawaskar, renowned experts in the treatment of scorpion stings, recommend that hyper-tension (due to Mesobuthus tamulus envenomation) be controlled by sublingual nifedipine, with peripheral venom action antagonised by the post-synaptic alpha-blocker prazosin.
Nifedipine reduces hypertension, and enhances
myocardial contractility caused by increased catecholamine levels. Prazosin
reduces preload and left ventricular impedence without heart rate or serum
renin increases. It also inhibits the suppression of insulin caused by
envenomation. Prazosin is also said to be useful in the treatment of pulmonary oedema
from scorpion envenomation.
·
Hypotension is treated with dopamine infusion, begin-ning at
a dose of 2 to 5 mcg/kg/min and increasing gradually to 20 mcg/kg/min, so as to
achieve and maintain systolic reading of around 90 mmHg.
·
Pulmonary oedema is treated with
prazocin or furo-semide (1 to 2 mg/kg IV every 4 to 6 hours) and oxygen.
Life-threatening pulmonary oedema may respond to a nitroprusside drip.
·
Agitation and convulsions can be
controlled with IV diazepam (5 to 10 mg, adults; 0.2 to 0.3 mg/kg, children;
repeated every 10 minutes as required). Alternatively, phenobarbitone can be
given, 5 to 10 mg/ kg IV.
·
Persistent vomiting usually responds
to metoclopramide 5 to 10 mg IV (adults), or 0.5 mg/kg (children).
·
Cardiac rhythm disturbances are
usually transient and resolve without specific treatment in most of the cases.
Persistent tachyarrhythmias can be reversed with propranolol (1 mg/dose IV,
administered no faster than 1 mg/min, repeated every 5 minutes until desired
response is seen, or a maximum of 5 mg has been given).
Antivenom
therapy—
o A
goat serum-derived antivenom has been avail-able in some countries since
several years, but there is controversy as to its efficacy. Most patients
develop serum sickness syndrome within 2 weeks of antivenom administration.
o Scorpion
antivenom effective against Mesobuthustamulus
has recently been introduced in India.* Therecommended dose is 1 vial
(reconstituted in 10 ml of injection water) initially, followed by further
doses if required.
Prevention of Scorpion Sting
·
Clear debris and rubbish from all areas of work or rest.
·
Repellents may be used in areas of scorpion infestation:
o
Spraying a mixture of 2% chlorine, 10% DDT and 0.2%
pyrethroid in an oil base is quite effective.
o
Alternatively, use a mixture of fuel oil, kerosene, and
small amounts of creosote.
·
Inspect shoes, clothing, and bedding for scorpions.
·
Do not reach into dark corners, receptacles, or boxes.
Use a flashlight first to check for
scorpions.
· As a rule, if one scorpion has been
encountered in a partic-ular area, there will be others around. Females
generally give birth to 50 to 60 young, which remain close to where they were
born. It is important to locate and kill them all.
Related Topics