Chapter: Modern Medical Toxicology: Organic Poisons (Toxins): Venomous Bites and Stings
Black Widow - Venomous Arachnids
Black Widow*
·
Widow (or hour-glass) spiders belong
to the Latrodectus species of phylum Arthropoda.
Other Common Names
·
Hourglass Spider.
Species
·
Latrodectus
mactans.
Physical Appearance
·
The widow spiders are cosmopolitan
and are found all over the world, except regions with extremes of climate
(polar regions, hot deserts, and high mountains). They are easily identified
because they are the only spiders with a black, globose abdomen.
·
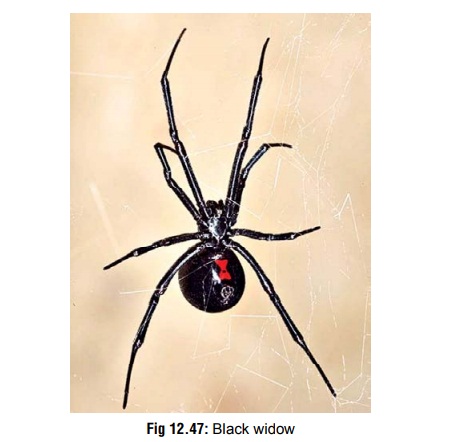
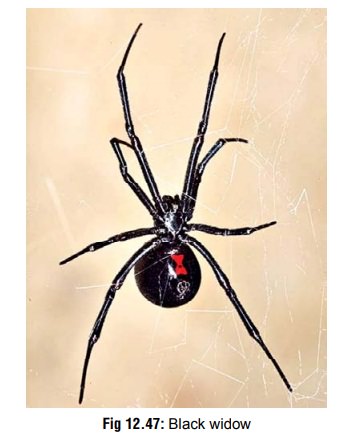
The female is much larger than the
male with a leg span of 5 cm and body length of 1.5 cm. It has a characteristic
red hourglass spot on the back of its shiny black body (Fig12.47). The male has more colourful white markings and isless
aggressive than the female. In fact, the popular name “Black Widow” is due to
the female’s practice of killing its partner after insemination.
·
The preferred habitats of these
spiders include outdoor toilets, stables, barns, woodpiles, and dark crevices.
They usually spin a somewhat irregular web in various corners of undisturbed
areas of homes or the outdoors.
·
The red-back spider (Latrodectus
hasselti) is best known from the adult female that usually has a black body
and legs, with the following distinctive markings on the abdomen: the dorsal or
top side has a distinct red stripe beginning in the mid portion, and on the
underside is a red area in the shape of an hourglass or two triangles. However,
variations on that pattern are common. The body may be light or dark brown;
there may be red markings in front of and beside the main red band which may be
light orange, or faded red. These spiders are found in open country areas, dark
places, rubbish heaps, wood heaps, stacks of bags, or of scrap metal, under the
bark of dead trees, empty tins, unused buckets, beneath or between stones,
behind ferns, near gas or water metres, old boxes, etc.
Venom
·
The venom of black widow is
neurotoxic, with six active components of molecular weight ranging from 5000–
130,000 D. The main component is alpha latrotoxin which binds avidly to a
specific presynaptic receptor.
·
The venom affects the motor
endplates of neuromuscular synaptic membranes by the binding of gangliosides
and glycoproteins at the synapses. This causes the channels for sodium influx
into neurons to remain open, as a result of which there is extensive release of
acetylcholine and noradrenaline into the synapses, thereby inhibiting
·
reuptake. The end result is massive
stimulation of motor endplates as the venom travels through the lymphatic
system.
Clinical Features (Latrodectism )
Grade 1
1. Sharp pain at bitesite, which may have one
or two small puncture wounds, 1 to 2 mm apart. The immediate area may be warm,
mildly indurated, and slightly reddened. Swelling of the affected part may
occur after red-back spider bites.
2. No systemic features.
Grade 2
1. Muscular pain in bitten extremity.
2. Extension of pain to the trunk.
3. Local diaphoresis of bitten extremity.
4. Tender regional lymphadenopathy may be present.
5.
No systemic features.
Grade 3
·
Generalised muscle pain and
weakness, with difficulty in walking.
·
Generalised sweating.
·
Tachycardia and hypertension are
quite common.
·
ECG changes have been reported in a
few victims: slur-ring of the QRS with ST and T segments depression, prolonged
QT interval, and changes consistent with inferolateral ischaemia.
·
Leucocytosis is a common finding.
·
Nausea, vomiting, and headache are
also very common.
·
Priapism, urinary retention, pyuria,
proteinuria, microscopic haematuria, and testicular pain have been reported in
a few cases.
·
During this period the victim often
displays a contorted, grimacing, sweating facial appearance, referred to as “facies latrodectismica”.
·
In severe cases, the following
manifestations occur: ptosis, salivation, hyperreflexia, tremor, convulsions,
tachypnoea, and respiratory compromise. Board-like rigidity of the abdomen,
shoulders, and back may develop. Although uncommon, acute renal failure has
been reported following envenomation. Death is uncommon, but is more likely in
the case of infants, old individuals, pregnant women, and chronic inva-lids.
Diagnosis
·
Leucocytosis
·
Elevated creatine kinase
·
Albuminuria.
Treatment
·
Calcium gluconate IV (10 ml of 10%) has been traditionally
advocated for pain relief, but its actual efficacy is doubtful.
·
Pain is usually better controlled
with a combination of IV morphine or pethidine and benzodiazepines (diazepam or
lorazepam). Milder cases may be treated with aspirin, paracetamol, and/or
codeine.
·
Application of cold or warm
compresses (as guided by patient comfort) to bitten site is usually helpful.
·
Swelling responds to non-steroidal
anti-inflammatory drugs.
·
Muscle relaxants such as diazepam,
methocarbamol, or dantrolene may help relieve muscle spasm.
·
Tetanus prophylaxis is essential.
·
Wound care:
o Cleansing
with antiseptics.
o Immobilisation,
elevation, and serial observation.
o If
infection sets in, antibiotics must be administered.
o Surgical
intervention (excision) may be necessary if lesion exceeds 4 cm at 12 hours
post-envenomation.
Related Topics