Chapter: Medical Surgical Nursing: Management of Patients With Coronary Vascular Disorders
Nursing Process: The Patient With Angina Pectoris
NURSING PROCESS: THE PATIENT WITH ANGINA PECTORIS
Assessment
The
nurse gathers information about the patient’s symptoms and activities,
especially those that precede and precipitate attacks of angina pectoris.
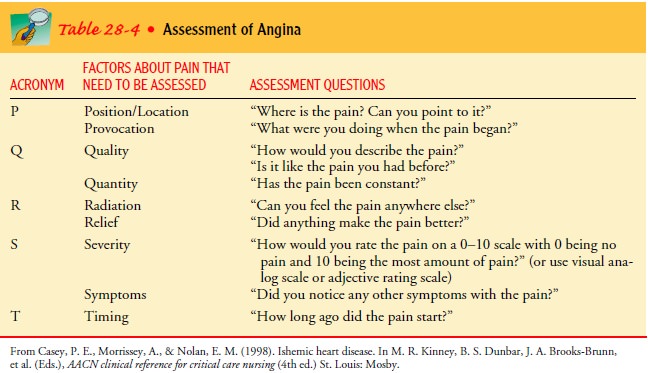
Appropriate questions are identified in Table 28-4, using a PQRST format. Other
helpful questions may be asked. How long does the angina usually last? Does
nitroglycerin relieve the angina? If so, how many tablets or sprays are needed
to achieve relief? How long does it takes for relief to occur?
The
answers to these questions form a basis for designing a log-ical program of
treatment and prevention. In addition to assessing angina pectoris or its
equivalent, the nurse also assesses the patient’s risk factors for CAD, the
patient’s response to angina, the patient’s and family’s understanding of the
diagnosis, and adherence to the current treatment plan.
Diagnosis
NURSING DIAGNOSES
Based
on the assessment data, major nursing diagnoses for the pa-tient may include:
·
Ineffective myocardial tissue
perfusion secondary to CAD, as evidenced by chest pain or equivalent symptoms
·
Anxiety related to fear of death
·
Deficient knowledge about the
underlying disease and methods for avoiding complications
·
Noncompliance, ineffective
management of therapeutic regimen related to failure to accept necessary
lifestyle changes
COLLABORATIVE PROBLEMS/ POTENTIAL COMPLICATIONS
Potential
complications that may develop include the following:
·
Acute pulmonary edema
·
Congestive heart failure
·
Cardiogenic shock
·
Dysrhythmias and cardiac arrest
·
MI (described later)
·
Myocardial rupture
·
Pericardial effusion and cardiac
tamponade
Planning and Goals
The
major patient goals include immediate and appropriate treat-ment when angina
occurs, prevention of angina, reduction of anxiety, awareness of the disease
process and understanding of the prescribed care, adherence to the self-care
program, and absence of complications.
Nursing Interventions
TREATING ANGINA
If
the patient reports pain (or the individual’s equivalent to pain), the nurse
takes immediate action. When a patient experiences angina, the nurse should
direct the patient to stop all activities and sit or rest in bed in a
semi-Fowler position to reduce the oxygen re-quirements of the ischemic myocardium.
The nurse assesses the pa-tient’s angina, asking questions to determine whether
the angina is the same as the patient typically experiences. A difference may
in-dicate a worsening of the disease or a different cause. The nurse then
continues to assess the patient, measuring vital signs and observing for signs
of respiratory distress. If the patient is in the hospital, a 12-lead ECG is
usually obtained and scrutinized for ST-segment and T-wave changes. If the
patient has been placed on cardiac monitoring with continuous ST-segment
monitoring, the ST segment is assessed for changes.
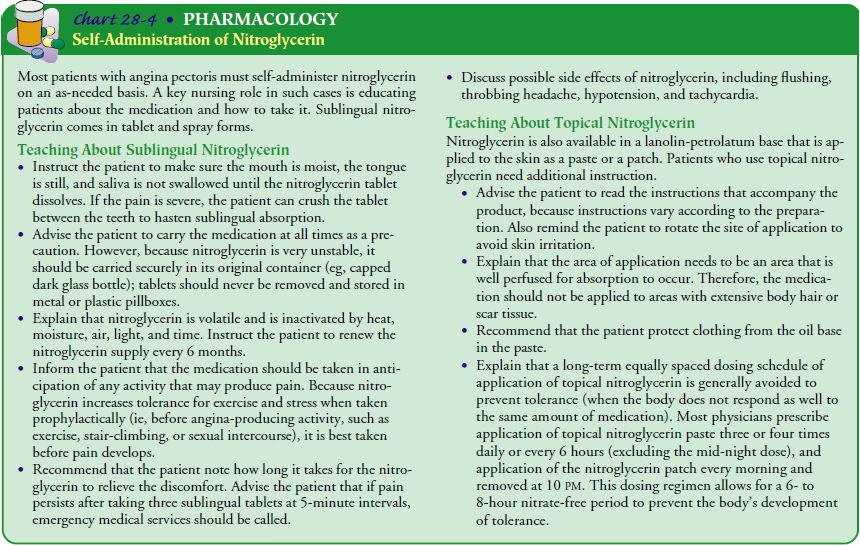
Nitroglycerin is administered sublingually, and the patient’s re-sponse is assessed (relief of chest pain and effect on blood pressure and heart rate). If the chest pain is unchanged or is lessened but still present, nitroglycerin administration is repeated up to three doses.
Each
time, blood pressure, heart rate, and the ST segment (if the patient is on a
monitor with ST segment monitoring capability) are assessed. The nurse
administers oxygen therapy if the patient’s respiratory rate is increased or
the oxygen saturation level is de-creased. Although there is no documentation
of its effect on out-come, oxygen is usually administered at 2 L/min by nasal
cannula, even without evidence of respiratory distress. If the pain is
signif-icant and continues after these interventions, the patient is usually
transferred to a higher-acuity nursing unit.
REDUCING ANXIETY
Patients
with angina often fear loss of their roles within society and the family. They
may also be fearful that the pain may lead to an MI or death. Exploring the
implications that the diagnosis has for the patient and providing information
about the illness, its treatment, and methods of preventing its progression are
im-portant nursing interventions. Various stress reduction methods should be
explored with the patient. For example, music therapy, in which patients are
given the opportunity to listen to selected music through headphones for a
predetermined duration, has been shown to reduce anxiety in patients who are in
a coronary care unit and may serve as an adjunct to therapeutic communi-cation
(Chlan & Tracy, 1999; Evans, 2002). Addressing the spir-itual needs of the
patient and family may also assist in allaying anxieties and fears.
PREVENTING PAIN
The
nurse reviews the assessment findings, identifies the level of activity that
causes the patient’s pain, and plans the patient’s ac-tivities accordingly. If
the patient has pain frequently or with minimal activity, the nurse alternates
the patient’s activities with rest periods. Balance of activity and rest is an
important aspect of the educational plan for the patient and family.
PROMOTING HOME AND COMMUNITY-BASED CARE
Teaching Patients Self-Care.
Learning about the modifiable riskfactors that contribute to the
continued development of CAD and resulting angina is essential. Exploring with
the patient and family what they see as their priority in managing the
disease and developing a plan based on their priorities can assist with patient
adherence to the therapeutic regimen. It is important to explore with the
patient methods to avoid, modify, or adapt the triggers for anginal pain. The
teaching program for the patient with angina is designed so that the patient
and family can explain the illness, identify the symptoms of myocardial
ischemia, state the actions to take when symptoms develop, and discuss methods
to prevent chest pain and the advancement of CAD. The goals of the educational
program are to reduce the frequency and severity of anginal attacks, to delay
the progress of the underlying disease, if possible, and to prevent any
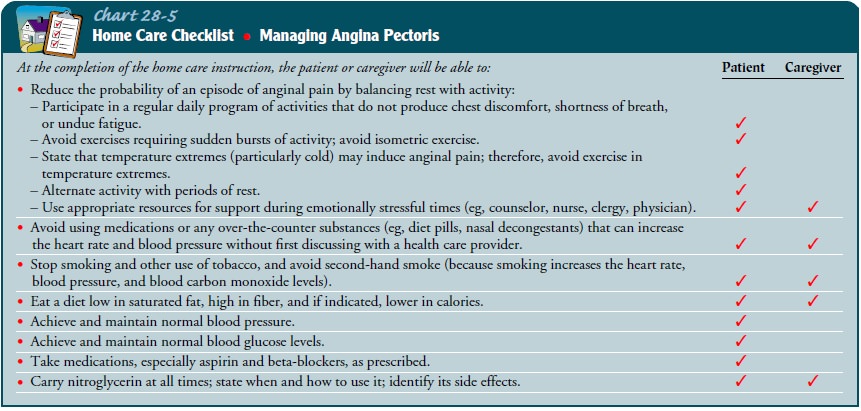
complications. The factors out-lined in the accompanying checklist Chart 28-5
are important in educating the patient with angina pectoris.
The
self-care program is prepared in collaboration with the patient and family or
friends. Activities should be planned to minimize the occurrence of angina
episodes. The patient needs to understand that any pain unrelieved within 15
minutes by the usual methods (see Chart 28-4) should be treated at the closest
emergency center; the patient should call 911 for assistance.
Evaluation
EXPECTED PATIENT OUTCOMES
Expected
patient outcomes may include:
1)
Reports that pain is relieved
promptly
a)
Recognizes symptoms
b)
Takes immediate action
c)
Seeks medical assistance if pain
persists or changes in quality
2)
Reports decreased anxiety
a)
Expresses acceptance of diagnosis
b)
Expresses control over choices
within medical regimen
c)
Does not exhibit signs and symptoms
that indicate a high level of anxiety
3) Understands ways to avoid complications and demonstrates freedom from complications
a)
Describes the process of angina
b)
Explains reasons for measures to
prevent complications
c)
Exhibits normal ECG and cardiac
enzyme levels
d)
Experiences no signs and symptoms of
acute MI
4)
Adheres to self-care program
a)
Takes medications as prescribed
b)
Keeps health care appointments
c)
Implements plan for reducing risk
factors
Related Topics