Chapter: Medical Physiology: Pregnancy and Lactation
Lactation
Lactation
Development of the Breasts
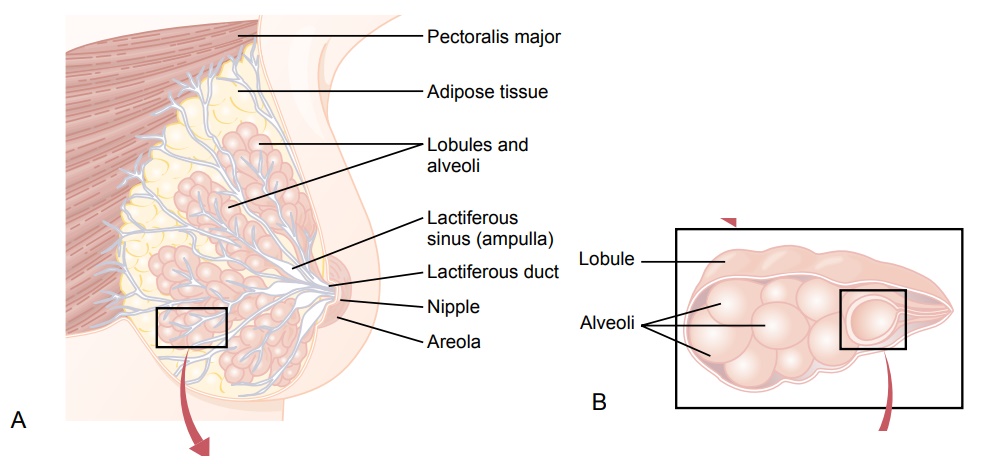
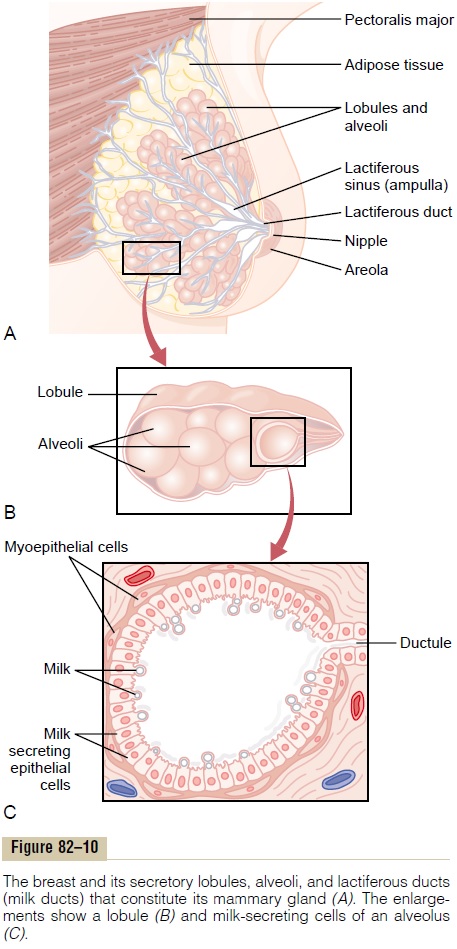
The breasts, shown in Figure 82–10, begin to develop at puberty. This development is stimulated by the estrogens of the monthly female sexual cycle; estro-gens stimulate growth of the breasts’ mammary glands plus the deposition of fat to give the breasts mass. In addition, far greater growth occurs during the high-estrogen state of pregnancy, and only then does the glandular tissue become completely developed for the production of milk.
Growth of the Ductal System—Role of the Estrogens. Allthrough pregnancy, the large quantities of estrogens secreted by the placenta cause the ductal system of the breasts to grow and branch. Simultaneously, the stroma of the breasts increases in quantity, and large quantities of fat are laid down in the stroma.
Also important for growth of the ductal system are at least four other hormones: growth hormone, pro-lactin, the adrenal glucocorticoids, and insulin.Each ofthese is known to play at least some role in protein metabolism, which presumably explains their function in the development of the breasts.
Development of the Lobule-Alveolar System—Role of Proges- terone. Final development of the breasts into milk-secreting organs also requires progesterone.Once the ductal system has developed, progesterone—acting synergistically with estrogen, as well as with the other hormones just mentioned—causes additional growth of the breast lobules, with budding of alveoli and development of secretory characteristics in the cells of the alveoli. These changes are analogous to the secretory effects of progesterone on the endometrium of the uterus during the latter half of the female menstrual cycle.
Initiation of Lactation—Function of Prolactin
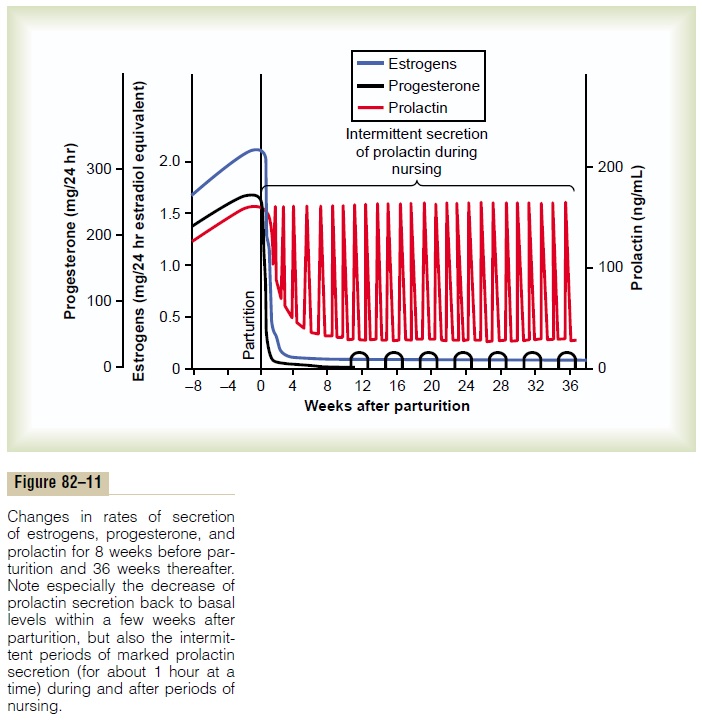
Although estrogen and progesterone are essential for the physical development of the breasts during preg-nancy, a specific effect of both these hormones is to inhibit the actual secretion of milk. Conversely, the hormone prolactin has exactly the opposite effect on milk secretion—promoting it. This hormone is secreted by the mother’s anterior pituitary gland, and its concentration in her blood rises steadily from the fifth week of pregnancy until birth of the baby, at which time it has risen to 10 to 20 times the normal nonpregnant level. This high level of prolactin at the end of pregnancy is shown in Figure 82–11.
In addition, the placenta secretes large quantities of human chorionic somatomammotropin, which proba-bly has lactogenic properties, thus supporting the pro-lactin from the mother’s pituitary during pregnancy. Even so, because of the suppressive effects of estrogen and progesterone, no more than a few milliliters of fluid are secreted each day until after the baby is born. The fluid secreted during the last few days before and the first few days after parturition is called colostrum; it contains essentially the same concentrations of pro-teins and lactose as milk, but it has almost no fat, and its maximum rate of production is about 1/100 the subsequent rate of milk production.
Immediately after the baby is born, the sudden loss of both estrogen and progesterone secretion from the placenta allows the lactogenic effect of prolactin from the mother’s pituitary gland to assume its natural milk-promoting role, and over the next 1 to 7 days, the breasts begin to secrete copious quantities of milk instead of colostrum. This secretion of milk requires an adequate background secretion of most of the mother’s other hormones as well, but most important are growth hormone, cortisol, parathyroid hormone, and insulin. These hormones are necessary to provide the amino acids, fatty acids, glucose, and calcium required for milk formation.
After birth of the baby, the basal level of prolactin secretion returns to the nonpregnant level over the next few weeks, as shown in Figure 82–11. However, each time the mother nurses her baby, nervous signals from the nipples to the hypothalamus cause a 10- to 20-fold surge in prolactin secretion that lasts for about 1 hour, which is also shown in Figure 82–11. This prolactin acts on the mother’s breasts to keep the mammary glands secreting milk into the alveoli for the subsequent nursing periods. If this prolactin surge is absent or blocked as a result of hypothalamic or pitu-itary damage or if nursing does not continue, the breasts lose their ability to produce milk within 1 week or so. However, milk production can continue for several years if the child continues to suckle, although the rate of milk formation normally decreases consid-erably after 7 to 9 months.
Hypothalamic Control of Prolactin Secretion. The hypothal-amus plays an essential role in controlling prolactin secretion, as it does for almost all the other anterior pituitary hormones. However, this control is different in one aspect: The hypothalamus mainlystimulates production of all the other hormones, but it mainly inhibits prolactin production. Consequently, damageto the hypothalamus or blockage of the hypothalamic-hypophysial portal system often increases prolactin secretion while it depresses secretion of the other anterior pituitary hormones.
Therefore, it is believed that anterior pituitary secre-tion of prolactin is controlled either entirely or almost entirely by an inhibitory factor formed in the hypo-thalamus and transported through the hypothalamic-hypophysial portal system to the anterior pituitary gland. This factor is called prolactin inhibitoryhormone. It is almost certainly the same as the cate-cholamine dopamine, which is known to be secreted by the arcuate nuclei of the hypothalamus and can decrease prolactin secretion as much as 10-fold.
Suppression of the Female Ovarian Cycles in Nursing Mothers for Many Months After Delivery. In most nursing mothers,the ovarian cycle (and ovulation) does not resume until a few weeks after cessation of nursing.The reason seems to be that the same nervous signals from the breasts to the hypothalamus that cause prolactin secretion during suckling—either because of the nervous signals themselves or because of a subsequent effect of increased prolactin—inhibit secretion of gonadotropin-releasing hormone by the hypothala-mus. This, in turn, suppresses formation of the pituitary gonadotropic hormones—luteinizing hormone and follicle-stimulating hormone. However, after several months of lactation, in some mothers, especially in those who nurse their babies only some of the time, the pituitary begins to secrete sufficient gonadotropic hormones to reinstate the monthly sexual cycle, even though nursing continues.
Ejection (or “Let-Down”) Process in Milk Secretion—Function of Oxytocin
Milk is secreted continuously into the alveoli of the breasts, but milk does not flow easily from the alveoli into the ductal system and, therefore, does not contin-ually leak from the breast nipples. Instead, the milk must be ejected from the alveoli into the ducts before the baby can obtain it. This is caused by a combined neurogenic and hormonal reflex that involves the posterior pituitary hormone oxytocin, as follows.
When the baby suckles, it receives virtually no milk for the first half minute or so. Sensory impulses must first be transmitted through somatic nerves from the nipples to the mother’s spinal cord and then to her hypothalamus, where they cause nerve signals that promote oxytocin secretion at the same time that they cause prolactin secretion.The oxytocin is carried in the blood to the breasts, where it causes myoepithelial cells (which surround the outer walls of the alveoli) to con-tract, thereby expressing the milk from the alveoli into the ducts at a pressure of +10 to 20 mm Hg. Then the baby’s suckling becomes effective in removing the milk. Thus, within 30 seconds to 1 minute after a baby begins to suckle, milk begins to flow. This process is called milk ejection or milk let-down.
Suckling on one breast causes milk flow not only in that breast but also in the opposite breast. It is espe-cially interesting that fondling of the baby by the mother or hearing the baby crying often gives enough of an emotional signal to the hypothalamus to cause milk ejection.
Inhibition of Milk Ejection. A particular problem innursing a baby comes from the fact that many psy-chogenic factors or even generalized sympathetic nervous system stimulation throughout the mother’s body can inhibit oxytocin secretion and consequently depress milk ejection. For this reason, many mothers must have an undisturbed puerperium if they are to be successful in nursing their babies.
Milk Composition and the Metabolic Drain on the Mother Caused by Lactation
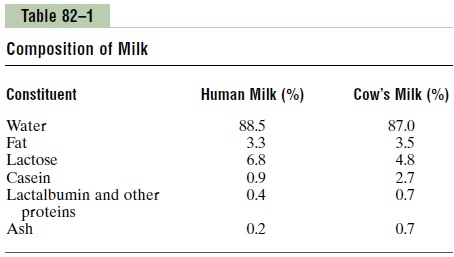
Table 82–1 lists the contents of human milk and cow’s milk. The concentration of lactose in human milk is about 50 per cent greater than in cow’s milk, but the concentration of protein in cow’s milk is ordinarily two or more times greater than in human milk. Finally, only one third as much ash, which contains calcium and other minerals, is found in human milk compared with cow’s milk.
At the height of lactation in the human mother, 1.5 liters of milk may be formed each day (and even more if the mother has twins). With this degree of lactation, great quantities of metabolic substrates are drained from the mother. For instance, about 50 grams of fat enter the milk each day, and about 100 grams of lactose, which must be derived by conversion from the mother’s glucose. Also, 2 to 3 grams of calcium phos-phate may be lost each day; unless the mother is drink-ing large quantities of milk and has an adequate intake of vitamin D, the output of calcium and phosphate by the lactating mammae will often be much greater than the intake of these substances. To supply the needed calcium and phosphate, the parathyroid glands enlarge greatly, and the bones become progressively decalci-fied. The mother’s bone decalcification is usually not a big problem during pregnancy, but it can become more important during lactation.
Antibodies and Other Anti-infectious Agents in Milk. Not onlydoes milk provide the newborn baby with needed nutrients, but it also provides important protection against infection. For instance, multiple types of anti-bodies and other anti-infectious agents are secreted inmilk along with the nutrients. Also, several different types of white blood cells are secreted, including both neutrophils and macrophages, some of which are especially lethal to bacteria that could cause deadly infections in newborn babies. Particularly important are antibodies and macrophages that destroy Escherichia colibacteria, which often cause lethal diar-rhea in newborns.
When cow’s milk is used to supply nutrition for the baby in place of mother’s milk, the protective agents in it are usually of little value because they are normally destroyed within minutes in the internal environment of the human being.
Related Topics