Chapter: Essentials of Psychiatry: Mental Disorders Due to a General Medical Condition
Klüver–Bucy Syndrome
Klüver–Bucy Syndrome
Definition
In 1939, KlĂĽver and Bucy (1939) noted some striking
behavio-ral changes in monkeys which had been subjected to bilateratemporal
lobectomy, and in so doing described the syndrome that now bears their names.
The full syndrome is characterized by hypermetamorphosis (excessive tendency to
take notice and attend and react to every visual stimulus), agnosia,
hyperorality, emotional placidity and hypersexuality. Some examples of the
syndrome in humans follow.
The first example demonstrates hypersexuality,
hyperoral-ity, agnosia and emotional placidity. The patient was a 31-year-old
woman, who, after recovering from a herpes simplex encephali-tis, “made
inappropriate sexual advances to female attendants, both manually and orally.
At home, she was constantly chew-ing and swallowing, and all objects within
reach were placed in her mouth…including toilet paper and faeces…Her affect was
characterized by passivity and a pet-like compliance with those attending her”
(Lilly et al., 1983).
The second example provides examples of
hypermeta-morphosis, hyperorality, agnosia and hypersexuality. The pa-tient, a
58-year-old man who had suffered from Alzheimer’s disease for 6 years, “spent
much of his time examining ordinary objects such as the doorstep, ashtrays, or
spots on the floor. He placed many objects in his mouth and occasionally ate
soil from plant containers … he rubbed his genitals so frequently that he
developed an excoriation on the shaft of his penis” (Lilly et al., 1983).
Finally, there is the case of a 46-year-old man,
who, during a complex partial seizure, “was observed grabbing for objects on
his bedside table, and he masturbated in front of the nurs-ing staff. He also
placed objects in his mouth, chewed on tissue paper, and attempted to drink
from his urine container” (Nakada et al.,
1984). Here, there are hypermetamorphosis, hypersexual-ity, hyperorality and
agnosia
Etiology and Pathophysiology
The various causes of the Klüver–Bucy syndrome are
listed in Table 33.11: in each case, bilateral damage or dysfunction of the
temporal lobes has occurred. The mechanism of such bilateral damage in the case
of precipitants is fairly straightforward. The neurodegenerative disorders
listed have a predilection for the temporal lobes, and this is particularly the
case in Pick’s dis-
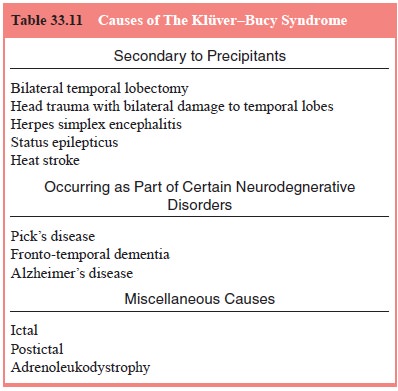
cause; in some cases, the syndrome itself may ease
and fronto-temporal dementia. Indeed, the appearance of the Klüver–Bucy
syndrome early in the course of a dementia is a significant diagnostic clue to
one of these two disorders; in the case of Alzheimer’s disease, the syndrome,
if it does occur, is generally seen only late in the course. Of the
miscellaneous causes, an ictal Klüver–Bucy syndrome is suggested by its
exqui-sitely paroxysmal onset and by the occurrence of other symptoms typical
for a complex partial seizure, such as confusion, and a postictal Klüver–Bucy
syndrome by the history of an immedi-ately preceding generalized seizure.
Adrenoleukodystrophy, the last in the list, is an extremely rare cause of the
Klüver–Bucy syndrome.
Assessment and Differential Diagnosis
The combination of hyperorality and hypersexuality
often brings the patient to medical attention: although the full syndrome
presents little diagnostic difficulty, as it is not mimicked by any other
condition, partial syndromes, consisting primarily of hy-permetamorphosis and
hypersexuality, may suggest mania. The differential rests on the presence or
absence of pressured speech and activity, findings typical of mania but absent
in the Klüver– Bucy syndrome.
Epidemiology and Comorbidity
The full Klüver–Bucy syndrome is, overall, rare; in
dementia clinics, however, full or partial Klüver–Bucy syndromes are commonly
seen.
Course
The course depends on the underlying have a fatal
outcome.
Treatment
The underlying cause, if possible, is treated. In
chronic cases, neuroleptics have been reported to be helpful; there are,
however, no controlled studies.
Related Topics