Chapter: Essentials of Psychiatry: Mental Disorders Due to a General Medical Condition
Anxiety Disorder Due to a General Medical Condition with Panic Attacks or with Generalized Anxiety
Anxiety Disorder Due to a General
Medical Condition with Panic Attacks or with Generalized Anxiety
Definition
Pathologic anxiety secondary to a general medical
condition may occur in the form of well-circumscribed and transient panic
at-tacks or in a generalized, more chronic form. As the differential diagnoses
for these two forms of anxiety are quite different, it is critical clearly to
distinguish between them.
Panic attacks have an acute or paroxysmal onset,
and are characterized by typically intense anxiety or fear which is
ac-companied by various “autonomic” signs and symptoms, such as tremor,
diaphoresis and palpitations. Symptoms rapidly cre-scendo over seconds or
minutes and in most cases the attack will clear within anywhere from minutes up
to a half-hour. Although attacks tend to be similar one to another in the same
patient, there is substantial interpatient variability in the symptoms seen.
Generalized anxiety tends to be of subacute or gradual on-set, and may last for long periods of time, anywhere from days to months, depending on the underlying cause. Here, some patients, rather than complaining of feeling anxious per se, may complain of being worried, tense or ill at ease. Autonomic symptoms tend not to be as severe or prominent as those seen in panic attacks: shakiness, palpitations (or tachycardia) and diaphoresis are per-haps most common.
Etiology and Pathophysiology
Panic attacks are most commonly seen in one of the
primary anxiety disorders, namely, panic disorder, agoraphobia, specific
phobia, social phobia, obsessive–compulsive disorder or post traumatic stress
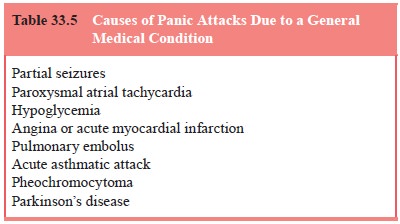
disorder, all of which are covered elsewhere in this book. The causes of
secondary panic attacks are listed in Table 33.5. Substance-induced anxiety
disorder related to drugs of abuse (e.g., cannibis, LSD) is covered in the
relevant substance-related disorders. Partial sei-zures and paroxysmal atrial
tachycardia are both characterized by their exquisitely paroxysmal onset, over
a second or two; in addition, paroxysmal atrial tachycardia is distinguished by
the prominence of the tachycardia and by an ability, in many cases, to
terminate the attack with a Valsalva maneuver. Hypoglycemia is often suspected
as a cause of anxiety, but before the diagnosis is accepted, one must
demonstrate the presence of “Whipple’s triad”: hypoglycemia (blood glucose #45
mg/dL), typical symp-toms, and the relief of those symptoms with glucose. Angina
or acute myocardial infarction can present with a panic attack, with the
diagnosis being suggested by the clinical setting, for example, multiple
cardiac risk factors. A pulmonary embolus, at the moment of its lodgment in a
pulmonary artery, may also present with a panic attack, and again here the
correct diagnosis is suggested by the clinical setting, for example,
situations, such as prolonged immobilization, which favor deep venous
throm-bosis. Acute asthmatic attacks are suggested by wheezing, and
pheochromocytoma by associated hypertension. Parkinson’s dis-ease patients
treated with levodopa may experience panic attacks during “off” periods.
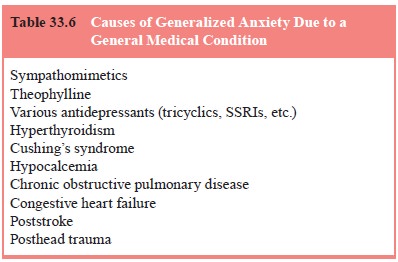
Generalized anxiety is most commonly seen in the
pri-mary psychiatric disorder, generalized anxiety disorder, and is discussed
elsewhere in this book. The secondary causes of gen-eralized anxiety are listed
in Table 33.6. Sympathomimetics and theophylline, as used in asthma and COPD,
are frequent causes, as are many of the antidepressants. Hyperthyroidism is suggested
by heat intolerance and proptosis, and Cushing’s syndrome by the typical
Cushingoid habitus (i.e., moon facies, hirsutism, acne, “buffalo hump” and
abdominal striae). Hypocalcemia may be suggested by a history of seizures or
tetany. Both chronic ob-structive pulmonary disease and congestive heart
failure are sug-gested by marked dyspnea. Stroke and severe head trauma may be
followed by chronic anxiety, but this is seen in only a minority of these
patients.
Assessment and Differential Diagnosis
Should one be fortunate enough to observe a patient during the panic attack, it is critical, in addition to carefully noting the spe-cific symptoms of the attack, to obtain vital signs, auscultate the heart and lungs, perform an EKG, and obtain blood for glucose and toxicology.
In
evaluating a patient who complains of chronic anxi-ety, it is important, before
deciding that this is, indeed, a case of pathologic generalized anxiety, first
to determine whether or not the patient has a depression, whether it be primary
or secondary: depression is often accompanied by anxiety, and such anxiety
clears upon adequate treatment of the depression. Assuming that the patient,
however, is not depressed, a work-up should include the following: auscultation
of the heart and lungs; CBC and liver enzymes (looking for the telltale
“alcoholic” combination of an elevated mean corpuscular volume and elevated
transaminases); thyroid profile; cortisol level and calcium level.
Epidemiology and Comorbidity
Although epidemiologic studies are lacking, the
clinical impres-sion is that anxiety secondary to a general medical condition
is common.
Course
This is determined by the underlying cause.
Treatment
Treatment is directed at the underlying cause, and
this is suf-ficient for all cases of secondary panic attacks and most cases of
secondary generalized anxiety: exceptions include poststroke and posthead
trauma anxiety, and in these cases benzodiazepines have been used with success.
Related Topics