Chapter: Essentials of Psychiatry: Mental Disorders Due to a General Medical Condition
Catatonic Disorder Due to a General Medical Condition
Catatonic Disorder Due to a
General Medical Condition
Definition
Catatonia exists in two subtypes, namely, stuporous
catatonia (also known as the akinetic or “retarded” subtype) and excited
catatonia, and each will be described in turn.
Stuporous catatonia is characterized by varying combi-nations of mutism, immobility and waxy flexibility; associated features include posturing, negativism, automatic obedience and “echo” phenomena. Mutism ranges from complete to partial: some patients may mumble or perhaps utter brief, often incom-prehensible, phrases. Immobility, likewise, ranges in severity: some patients may lie in bed for long periods, neither moving, blinking or even swallowing; others may make brief movements, perhaps to pull at a piece of clothing or to assume a different posture. Waxy flexibility, also known by its Latin name, cerea fl exibilitas, is characterized by a more or less severe “lead pipe” rigidity combined with a remarkable tendency for the limbs to stay in whatever position they are placed, regardless of whether the patient is asked to maintain that position or not. Posturing is said to occur when patients spontaneously assume more or less bizarre postures, which are then maintained: one patient crouched low with his arm wrapped over his head, another stood with one arm raised high and the other stuffed inside his belt. Negativism entails a mulish, intractable and automatic resistance to whatever is expected, and may be either “passive” or “active”. Passively negativistic patients simply fail to do what is asked or expected: if clothes are laid out they will not dress; if asked to eat or take pills, their lips remain frozen shut. Active negativism manifests in doing the opposite of what is expected: if asked to come into the office, the patient may back into the hallway or if asked to open the eyes wide to allow for easier examination, they may cramp the eyes closed. Automatic obedience, as may be sus-pected, represents the opposite of negativism, with affected pa-tients doing exactly what they are told, even should it place them in danger. Echo phenomena represent a kind of automatic obedi-ence: in echolalia patients simply repeat what they hear and in echopraxia they mimic the gestures and activity of the examiner.
It should be noted that in negativism, automatic
obedience and echo phenomena there is nothing natural or fluid about the
pa-tient’s behavior. To the contrary, movements are often awkward, wooden and
tinged with the bizarre.
Excited catatonia manifests with varying degrees of
bi-zarre, frenzied and purposeless behavior. Such patients typically keep to
themselves: one marched in place, all the while chant-ing and gesticulating;
another tore at his hair and clothing, broke plates in a corner then crawled
under the bed where he muttered and thrashed his arms.
Etiology and Pathophysiology
Stuporous catatonia, in the majority of cases,
occurs as part of such primary psychiatric disorders as schizophrenia or a
depressive epi-sode of either major depression or bipolar disorder, and these
are discussed elsewhere in this text. The causes of catatonia due to a general
medical condition or medications are listed in Table 33.8.
Stuporous catatonia occurring in association with
epilepsy is often suggested by a history of grand mal or complex partial
seizures. Ictal catatonia is further suggested by its exquisitely par-oxysmal
onset, and postictal catatonia by an immediately preced-ing “flurry” of grand
mal or complex partial seizures. Psychosis of forced normalization is an
interictal condition distinguished by the appearance of symptoms subsequent to
effective control of seizures. The chronic interictal psychosis is also, as
suggested by the name, an interictal condition which, however, appears not
after seizures are controlled but rather in the setting of ongoing, chronic uncontrolled
epilepsy. Of medications capable of caus-ing catatonia, neuroleptics are by far
the most common. Viral
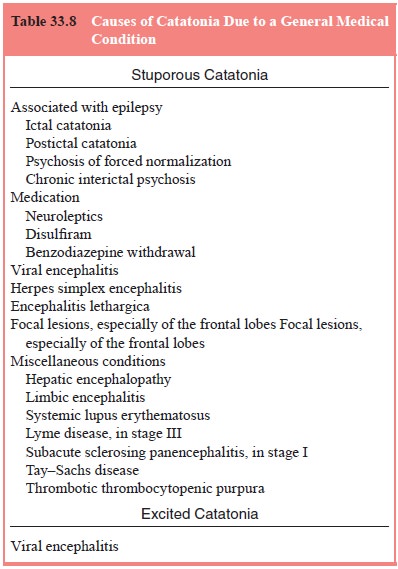
encephalitis is suggested by concurrent fever and
headache: her-pes simplex encephalitis should always be considered in such cases,
given its treatability; further it must be kept in mind that although
encephalitis lethargica no longer occurs in epidemics, sporadic cases do still
occur. Focal lesions capable of causing catatonia are typically found in the
medial or inferior portions of the frontal lobes. The miscellaneous conditions
listed are all quite rare causes of catatonia.
Excited catatonia, in the vast majority of cases,
is caused by either schizophrenia or bipolar disorder (during a manic
epi-sode): only rarely is it seen due to a general medical condition, as for
example, a viral encephalitis.
Assessment and Differential Diagnosis
Stuporous catatonia must be distinguished from
akinetic mut-ism and from stupor of other causes. Akinetic mutes appear quite
similar to immobile and mute catatonics: akinetic mutes, however, lack such
signs as waxy flexibility, posturing and negativism, all of which are typically
seen in catatonia. Stupor of other causes is readily distinguished from
catatonic stupor by the salient fact that catatonics remain alert, in stark
contrast with the somnolence or decreased level of consciousness seen in all
other forms of stupor.
Excited catatonia must be distinguished from mania.
Mania is typified by hyperactivity, which at times may be quite frenzied: the
difference with catatonia is that patients with ma-nia want to be involved,
whereas those with catatonia keep to themselves; as Kraepelin (Bear et al., 1982) noted, in catatonia “the
excitement, even when extremely violent, frequently takes place within the smallest space …. The patients have not
as a rule any tendency to influence their surroundings, but their restless-ness
exhausts itself in wholly aimless activity…”.
Epidemiology and Comorbidity
Stuporous catatonia due to a general medical
condition overall is, in general, a rare condition.
Course
This is determined by the course of the underlying
cause.
Treatment
In addition to treating, if possible, the
underlying cause, cata-tonia may be symptomatically relieved by lorazepam given
parenterally in a dose of 2 mg; in severe cases wherein lorazepam is not
sufficiently effective and the patient is at immediate risk, consideration
should be given to emergency ECT, which is typi-cally dramatically effective,
generally bringing relief after but a few treatments.
Related Topics