Chapter: Biology of Disease: Infectious Diseases and Treatments
Infections of the Respiratory System
INFECTIONS OF THE RESPIRATORY
SYSTEM
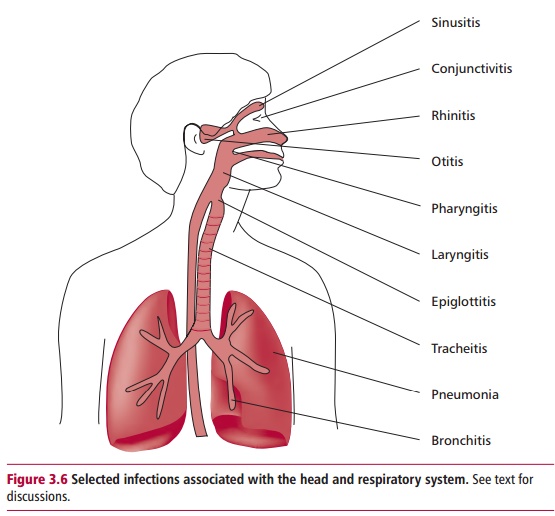
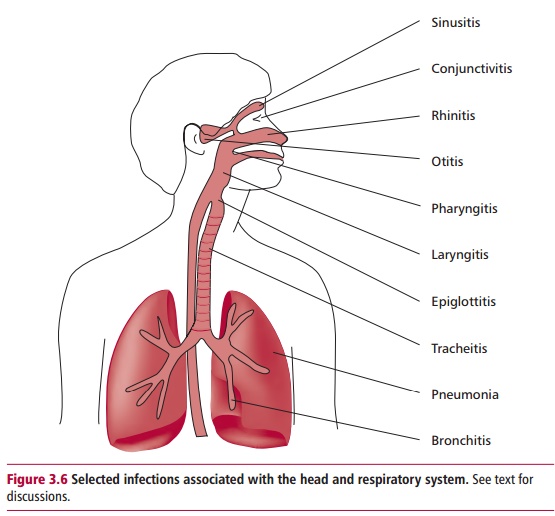
The respiratory system is constantly exposed to
inhaled microorganisms but is protected by extensive defenses. The nose filters
out particles larger than 10 Lm although those smaller than 5 Lm may reach the bronchi and
alveoli. Inaddition, there is a host of immune defenses including alveolar
macrophages, secretory IgA antibodies, complement proteins, surfactant
proteins, secreted defensins and lactoferrin . Despite this, infections of the
respiratory tract are frequent causes of illness. The World Health Organization
(WHO) has reported that many hundreds of millions of patients suffer acute
infections of the lower respiratory tract worldwide. Figure 3.6 indicates the sites of a number of respiratory diseases.
Respiratory viruses are transmitted directly by
aerosols or indirectly from contaminated surfaces. The first site of attack is,
not surprisingly, the epithelium of the nose and throat. Indeed, the hundreds
of corona and rhinoviruses that cause the common cold replicate at 32 to 33oC, the
temperature of the mucosal surface lining the nose. The influenza viruses (Figures 2.4 and 2.8) infect and replicate in respiratory epithelial cells causing
cellular damage. The generalized symptoms that present, such as muscular aches,
malaise and anorexia, suggest the virus may spread systemically from the
respiratory tract but there is no conclusive evidence for this.
The loss of ciliated and mucus producing epithelial
cells impairs clearance of invading microbes and creates conditions for
secondary bacterial infections of staphylococci, streptococci or Haemophilus influenzae. Bacterial
proteases, for example the V8 protease of Staphylococcus
aureus, can enhance the infectiveness of the influenza virus by improving
virus adhesion.
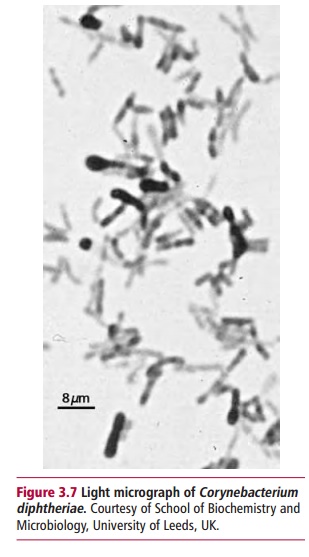
Corynebacterium
diphtheriae (Figure 3.7)
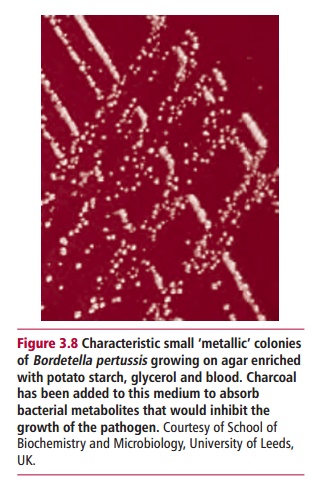
and Bordetella pertussis (Figure 3.8) are obligate bacterial
pathogens. Corynebacterium diphtheriae infectsthe
nasopharynx and the tonsils and may lead to a lethal systemic infection
affecting the heart, liver and kidneys. Bordetella
pertussis is the causative agent of whooping cough. It adheres to the
epithelial cells lining the trachea and bronchi where it interferes with
ciliary action and releases toxins and substances that damage and kill cells
and irritate the surface, causing the characteristic cough. Effective vaccines
are available against both organisms although 40 million infections of whooping
cough occur annually worldwide. In contrast, Streptococcus pneumoniae, Haemophilus
influenzae, Staphylococcusaureus and Moraxella catarrhalis, make up to 60%
of the normal bacterialpopulation of the nasopharyngeal mucous membrane in
healthy individuals. They can become opportunistic pathogens in immunosuppressed
individuals or following changes to the bacterium that render it increasingly
virulent. The commonest form of bacterial pneumonia is lobar pneumonia caused
by Streptococcus pneumoniae and
results in a massive inflammation of one lobe of the lung. Staphylococcus aureus may cause bronchopneumonia, while Haemophilus influenzae can infect the
epiglottis.
Mycobacterium
tuberculosis (Figure 3.9)
causes tuberculosis (TB) of the lungand may be considered a rather special case
of bacterial infection of the lower respiratory tract. The bacteria enter the
alveoli in inhaled air and are phagocytozed by macrophages where they escape
being killed and multiply . Mycobacteria can then enter the lymphatic system
and invade a neighboring lymph node. The healing of local lesions leads to
calcification of the lung tissues. In immunodeficient individuals, the lymph
nodes and tissues may be progressively affected until eventually the
mycobacteria are spread by the blood. Also with impaired immunity, dormant Mycobacteriumtuberculosis can be
reactivated causing a severe form of pneumonia.
Atypical pneumonias can result from infections with Mycoplasmapneumoniae, Chlamydia pneumoniae and Legionella pneumophila. Theseinfections
are associated with ‘flu-like' symptoms, such as high temperatures and
coughing, although bronchial secretions and sputum do not contain pus as would
be expected of a typical bacterial lobar pneumonia.
Generally, pathogenic fungi do not produce toxins but
damage tissues directly or disturb normal metabolic functions and can induce
hypersensitivity responses . Fungi can cause respiratory infections; Aspergillus fumigatus can invade the
respiratory system and lead to one of several types of diseases. It may simply
grow in the mucus of the bronchi and induce a hypersensitive state but may
invade old wound cavities of the lungs, such as those resulting from TB, and
grow as a solid mass called an aspergilloma.
Aspergillosis may also result from an invasive growth in the lungs and other
tissues. Generally, the infective dose of spores is extremely large although
the invasive form may be secondary to other systemic diseases. Similarly, Pneumocystis carinii can cause a serious
pneumonia (PCP) in AIDS compromized patients. The yeast, Candida albicans, is also an opportunistic agent in sufferers of
AIDS.
Related Topics