Chapter: Basic Radiology : Imaging of the Heart and Great Vessels
Exercise: Monitoring Devices
EXERCISE 3-6.
MONITORING DEVICES
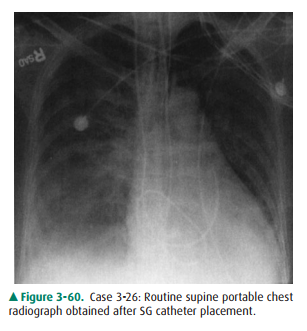
3-26. The complication of
Swan-Ganz catheter placement in Case 3-26 (Figure 3-60) is
A.
malposition of the tip.
B.
pneumothorax.
C.
perforation.
D.
catheter coiling.
E.
catheter thrombosis.
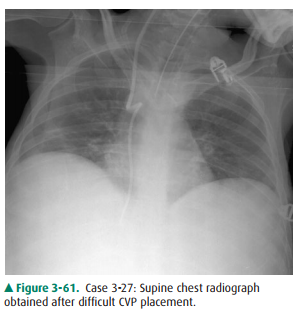
3-27. The tip of the
central venous catheter in Case 3-27 (Figure 3-61) is in the
·
inferior vena cava.
·
right ventricle.
·
azygous vein.
·
hemiazygous vein.
·
middle hepatic vein.
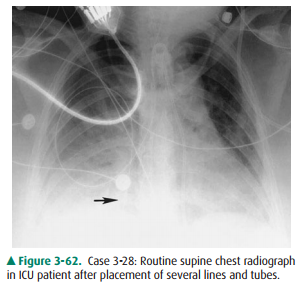
3-28. The malpositioned
catheter in Case 3-28 (Figure3-62) is a(n)
A.
tracheostomy tube.
B.
intraaortic balloon pump.
C.
Swan-Ganz catheter.
D.
nasogastric tube.
E.
Blakemore tube.
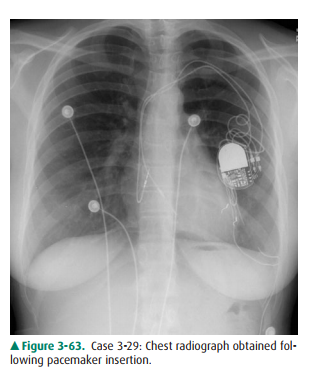
3-29. The complication
with the pacemaker shown in Case 3-29 (Figure 3-63) is
A.
right atrial lead dislodgement.
B.
right ventricular perforation.
C.
pneumothorax.
D.
right ventricular lead dislodgement.
E.
diaphragmatic pacing.
3-30. The catheter in
Case 3-30 (Figure 3-64, arrow) is in the
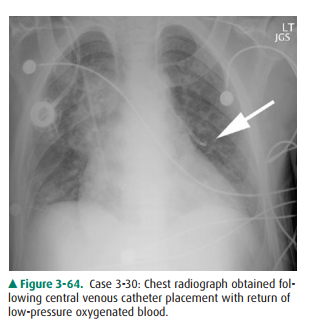
A.
lung parenchyma.
B.
left superior vena cava.
C.
left upper lobe pulmonary vein.
D.
descending thoracic aorta.
E.
left pulmonary artery.
Radiographic Findings
3-26. The supine portable
chest radiograph obtained after SG catheter placement in this case (Figure
3-60) is coiled within the right ventricle before it terminates in the proximal
main pulmonary artery (D is the cor-rect answer to Question 3-26). This coiling
of the catheter in the right ventricle may cause thrombosis or arrhythmia, and
it is necessary to reposition this catheter.
3-27. The supine chest
radiograph in this case (Figure 3-61) shows two turns in the course of the
catheter after a difficult CVP placement. The catheter turns posteri-orly into
the azygous vein and then descends on the right in the hemiazygous system (D is
the correct answer to Question 3-27).
3-28. In this case
(Figure 3-62), the chest radiograph ob-tained shows a nasogastric tube
extending down the right main bronchus into the right lung (Figure 3-62, arrow)
(D is the correct answer to Question 3-28).
3-29. In this case
(Figure 3-63), the tip of the right ventric-ular pacemaker lead does not extend
to the expected border of the myocardium. Usually a slight shoul-dering is
encountered as the lead crosses the tricus-pid valve. In some cases, the right
ventricular lead may be positioned higher along the interventricular septum and
may take a more horizontal course. A vertical course, as in this case,
indicates the tip is not lodged in the myocardium. This positioning results in
a lack of normal pacing function. The right atrial lead is in an appropriate
position. (D is the correct answer to Question 3-29.) midline to the superior
vena cava, extends into the left superior pulmonary vein (C is the correct
answer to Question 3-30). Because it is carrying blood returning from the
pulmonary capillary bed, it is oxygenated like systemic arterial blood, but
comes from a low-pressure system.
Discussion
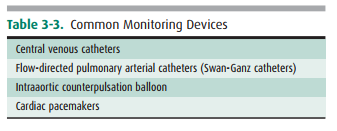
As mentioned in the subsection on
monitoring devices, a variety of catheters can be inserted into the heart and
great vessels to monitor various hemo-dynamic parameters, particularly in the
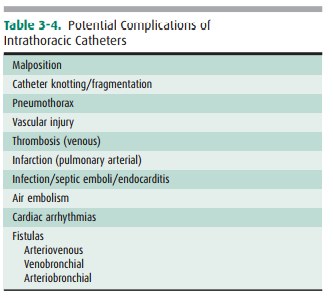
ICU setting. Table 3-3 lists the most common monitoring devices, and Table 3-4
shows the most common complications from place-ment of these devices. It is
important to trace out and ac-count for each catheter individually. For
instance, the nasogastric tube might have initially been mistaken for an ECG
lead. The result of instilling fluid through this tube could have been
disastrous. Even so, the result of this place-ment was a pneumothorax. We have
reviewed the normal placement of catheters and some of the more common re-lated
complications.
Related Topics