Chapter: Basic Radiology : Imaging of the Heart and Great Vessels
Exercise: Heart And Great Vessel Calcifications
EXERCISE 3-5.
HEART AND GREAT VESSEL CALCIFICATIONS
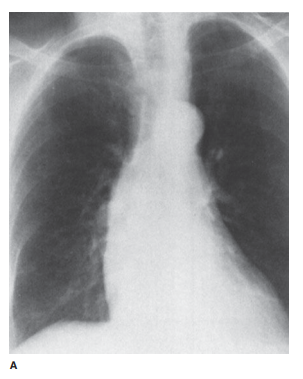
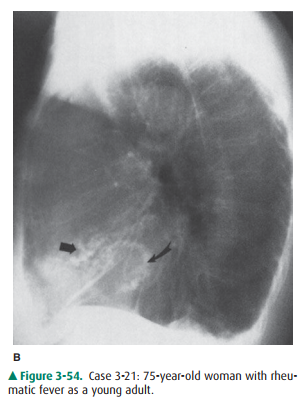
3-21. In Case 3-21
(Figure 3-54) the calcific density (straight arrow( is due to calcification of
the
A.
A,mitral valve
B.
B, tricuspid valve
C.
C, aorta valve
D.
D, pulmonary embolusy
E.
E, pericardium
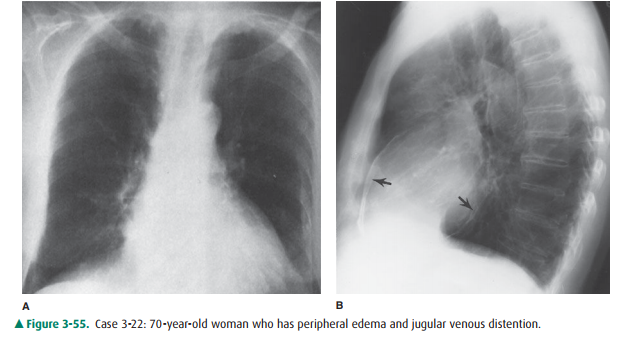
3-22. In Case 3-22
(Figure 3-55) the calcification are related to
A, pulmonary arteries
B, pericardium
C, mycocardium
D, ascending aorta
.E, descending thoracic aorta
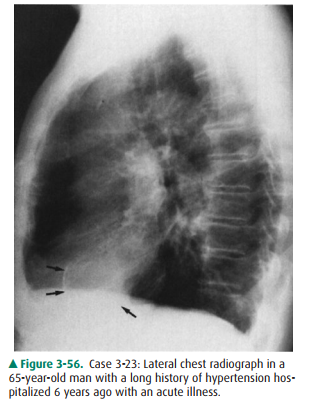
3-23. In Case 3-23
(Figure 3-56) the calcification on the chest radio graph are related to which
structure?
A,Pericardium
B,Mitral valve
C,Aortic valve
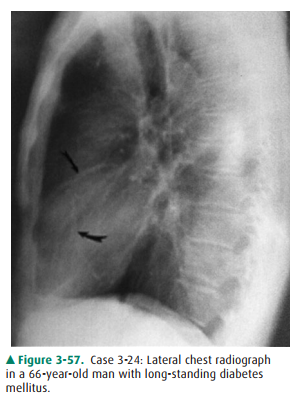
3-24. In Case 3-24
(Figure 3-57) the curved arrows point to calcification within the region of
which cardiac structure?
A. Aortic valve
B.Mitral valve
C. Pericardium
D. Coronary artery
E.Aortic aneurysm
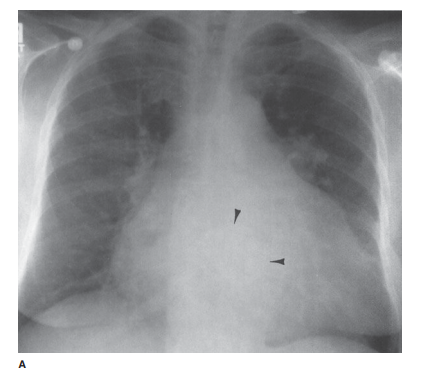
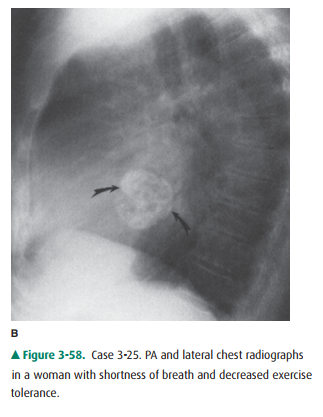
3-25. In Case 3-25
(Figure 3-58) the arrows and arrow-heads point to a(n)
A.
calcified mediastinal mass.
B. calcified left atrial myxoma.
C. pulmonary embolus calcification.
D.
aortic valve calcification.
E.
mitral valve calcification.
Radiographic Findings
3-21. The PA and lateral
chest radiographs (Figure 3-54) show curvilinear coarse calcifications in the
mitral an-nulus (curve arrow) and linear calcification (straight arrow) reside
in the aortic value, best seen on the lateral projection (C is the correct
answer to Question 3-21).
3-22. This case (Figure
3-55) shows pericardial calcifica-tion in a woman who had viral pericarditis as
a young child (B is the correct answer to Question 3-22). Note that the
calcification is seen much better on the lat-eral view.
3-23. The chest
radiograph in this case (Figure 3-56) shows linear calcification (arrows) in a
focal area overlying the left ventricle. This calcification resides in a left
ventricular aneurysm that this man developed after a myocardial infarction 6
years earlier (E is the correct answer to Question 3-23).
3-24. The lateral chest
radiograph in this case (Figure 3-57) shows linear tram-track calcifications
overlying the course of the coronary arteries. These calcifications represent
coronary artery atherosclerosis in a patient with long-standing diabetes (D is
the correct answer to Question 3-24).
3-25. In this case
(Figure 3-58), a circular, heavily calcified area overlying the left atrium is
seen in both the PA (arrowheads) and lateral (curved arrows) projec-tions.
These calcifications resided within a left atrial myxoma that was causing the
patient’s symptoms of shortness of breath and decreased exercise tolerance (B
is the correct answer to Question 3-25).
Discussion
Calcifications, present in almost
any area of the cardiovascu-lar system, may be either metastatic or dystrophic
in origin. Metastatic calcifications are usually caused by soft-tissue
deposition of calcium due to hypercalcemia of any cause. Dy-strophic
soft-tissue calcifications are responses to tissue in-jury or degeneration and
have no metabolic cause. They can be seen in practically any of the soft-tissue
components of the cardiovascular system. We concentrate -ventional chest
radiograph is within the aorta, usually in elderly patients with long-standing
atherosclerotic disease or di-abetes. In this instance, the calcification is
linear and is asso-ciated with the aortic wall. These calcifications may also
be present in aneurysms (see Figure 3-34).
The aortic valve and mitral valve
annulus are the most common intracardiac regions to demonstrate dystrophic
cal-cification, usually secondary to long-standing stenosis or in-sufficiency
from rheumatic fever. Bicuspid valves may also show this type of calcification.
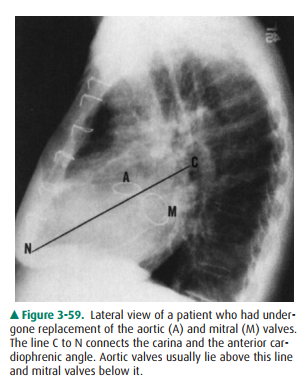
The lateral film is best for de-ciding which valve is calcified. A line drawn
from the hilumobliquely and downward to intersect the anterior cardio-phrenic
angle (N) will project behind aortic calcifications (A) (Figure 3-59).
Calcifications that lie in back of this line are usually mitral annulus
calcifications (M) (Figure 3-59). The presence of mitral annular calcification
has been shown to predict the presence of carotid atherosclerosis and therefore
may be associated with stroke.
Pericardial calcification as in
Case 3-22 (Figure 3-55) is seen in approximately 50% of patients with
constrictive peri-carditis. It has a characteristic curvilinear appearance
outlin-ing the location of the pericardium and is most often seen along the
right heart border (Figure 3-55).
Myocardial calcification, as is
seen in left ventricular aneurysms, was discussed in the exercise on altered
cardiac contour and is shown in a slightly different form in Case 3-23 (Figure
3-56). Thin, focal, linear calcifications overlying the left ventricle should
be considered as aneurysms, and echocardiography, CT, and MR imaging are all
useful exami-nations to confirm this diagnosis.
Calcifications within the wall of
the coronary arteries, as exhibited in Case 3-24 (Figure 3-57), are recognized
on con-ventional radiographs as thin, linear, calcific deposits corre-sponding
to the course of the coronary arteries. When discovered by conventional
radiographs, it is a late finding of atherosclerosis, and these patients have a
high incidence of obstructive coronary artery disease.
Case 3-25 (Figure 3-58) is an
example of the rare pri-mary cardiac neoplasm that may calcify and be detected
ini-tially on the plain film. The cardiac tumor that most commonly calcifies is
the left atrial myxoma, and calcifica-tion occurs in about 10% of these lesions
(Figure 3-58). Rarely, myocardial metastatic disease (such as osteosar-coma) or
other primary cardiac tumors may calcify. Finally, primary mediastinal
neoplasms such as teratomas may rarely show calcification. In these patients,
CT should be performed for diagnosis.
Related Topics