Chapter: Basic Radiology : Brain and Its Coverings
Exercise: Intracranial Vascular Abnormalities
EXERCISE 12-6.
INTRACRANIAL VASCULAR ABNORMALITIES
12-14. In Case 12-14, what is the reason
for the abnormality on the CT scan (Figure 12-34 A–C)?
A.
Cerebral aneurysm
B.
Arteriovenous malformation
C.
Head trauma
D.
Carotid dissection
12-15. In Case 12-15, what is the reason for the abnormality on
the CT scan (Figure 12-35 A-C)?
A.
Cerebral aneurysm
B.
Arteriovenous malformation
C.
Head trauma
D.
Carotid dissection
E.
Vasculitis
Radiologic Findings
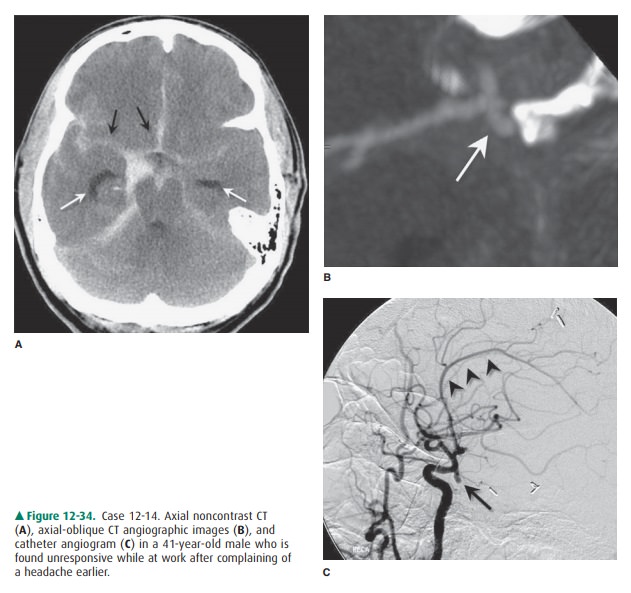
12-14. In this case, the CT scan (Figure 12-34 A) shows
exten-sive subarachnoid hemorrhage filling the basal cis-terns, more pronounced
on the right (black arrows), with extension of hemorrhage into the
interhemi-spheric and Sylvian fissures. Enlargement of the tem-poral horns
(white arrows) is indicative of early hydrocephalus. An oblique craniocaudal
view from a CT angiogram (Figure 12-34 B) shows a 4-mm saccu-lar aneurysm
arising from the right paraclinoid inter-nal carotid artery (arrow), most
likely posterior communicating artery origin. A lateral view taken from a right
common carotid catheter angiogram (Figure 12-34 C) confirms a posterior
communicating artery origin aneurysm (black arrow) with upward distortion of
the normal anterior cerebral artery con-figuration secondary to hydrocephalus
(black arrow-heads). (A is the correct answer to Question 12-14.)
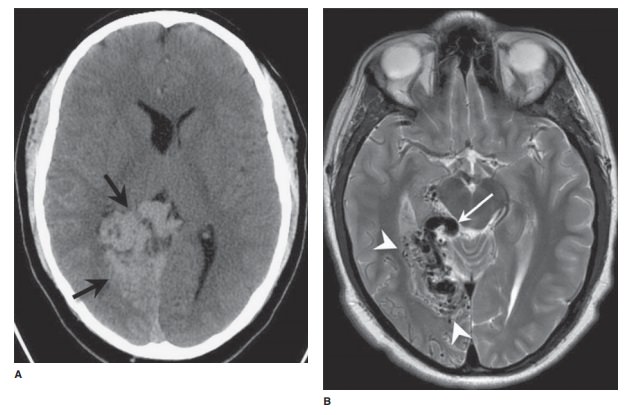
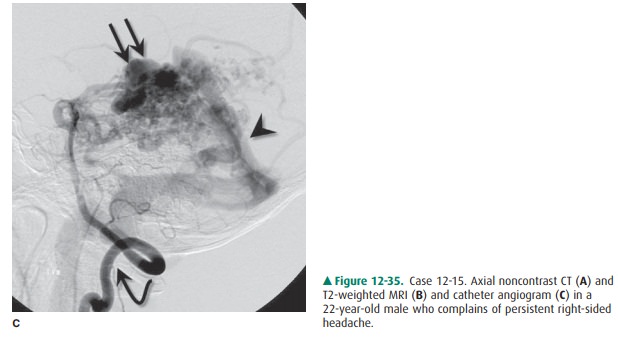
12-15. In this case, the noncontrast
CT scan (Figure 12-35 A) shows a lobulated, hyperdense mass (black arrows)
centered in the medial right occipital lobe with ef-facement of the right
occipital horn. Accompanying axial T2 MRI (Figure 12-35 B) reveals a nidus of
low signal vascular “flow-voids” (white arrowheads) in the occipital lobe with
a more prominent draining vein extending into the quadrigeminal plate cistern
(white arrow). A subsequent catheter angiogram (Figure 12-35 C) of the right
vertebral artery (curved arrow) confirms a high-flow vascular lesion with a
tangle of vessels (double black arrows) and early ve-nous opacification
(arrowhead) characteristic of an arteriovenous malformation. (B is the correct
answer to Question 12-15.)
Discussion
Cerebrovascular disorders (strokes)
were discussed in Exer- cise 12-2, which dealt
mainly with cerebral infarction second- ary to atherosclerosis. For
information on other causes of other
common vascular conditions
affecting the CNS: aneurysms and vascular malformationsbeen
thought to develop at congenitally weak areas of a blood vessel wall. Recent
evidence, however, has questioned this view, and many now believe that saccular
aneurysms are probably acquired lesions from abnormal hemodynamic stresses that
damage the arterial wall.
Intracranial aneurysms are
usually asymptomatic until they rupture, at which time the patient typically
presents with a severe headache resulting from subarachnoid hemor-rhage. The
vast majority of nontraumatic SAHs occur as a result of aneurysm rupture. CT is
very good at demonstrating SAH. Patients usually undergo CT angiography
whenever nontraumatic SAH is detected, and occasionally cerebral
ar-teriography.
Common locations for intracranial
aneurysms include the anterior communicating artery, the internal carotid
ar-tery at the origin of the posterior communicating artery, and the middle
cerebral artery trifurcation. Posterior fossa aneurysms are less common; they
make up only around 10% of all intracranial aneurysms and typically arise from
the basilar artery tip.
Vascular malformations can be
divided into four major types: true arteriovenous malformations (as
demonstrated in Case 12-15), cavernous hemangiomas, venous angiomas, and
capillary telangiectasias. AVMs are congenital lesions consist-ing of a tangle
of abnormal blood vessels, usually within the brain parenchyma, that are fed by
enlarged cerebral arteries and drained by dilated, tortuous veins. Because
there is no normal intervening brain parenchyma for the blood to flow through,
blood is rapidly shunted from the arterial to the ve-nous side. This shunting
is dramatically demonstrated on cerebral arteriography. Patients with AVMs
usually present with intracranial hemorrhage or seizures. MR imaging or
contrast-enhanced CT can demonstrate the tortuous vascu-lar channels of most
AVMs, although cerebral arteriography is the definitive study in this
condition.
The other intracranial vascular
malformations have very characteristic appearances on MR imaging, although they
are frequently invisible on cerebral arteriography. Patients with these
“low-pressure” malformations can present with headaches, seizures, or, rarely,
intracranial hemorrhage. Many of these lesions, however, are incidentally
discovered on MR scans performed for other reasons.
Related Topics