Chapter: Basic Radiology : Brain and Its Coverings
Exercise: Intracranial Infections
EXERCISE 12-4.
INTRACRANIAL INFECTIONS
12-9. In Case 12-9, what is the most likely diagnosis (Figure
12-25 A, B)?
A.
Frontal contusion
B.
Aneurysm with intraventricular hemorrhage
C.
Parietal lobe abscess
D.
Intracranial lymphoma
E.
Cerebritis
12-10. In Case 12-10, the location of the abnormality is
pathognomonic for which type of infection (Figure 12-26 A, B)?
A.
Toxoplasmosis
B.
Tuberculosis
C.
Cryptococcus
D. Herpes Staphylococcus
12-11. In Case 12-11, the major differential diagnosis for this
lesion is toxoplasmosis versus (Figure 12-27)
A.
Cryptococcus
B.
Intracranial lymphoma
C.
Sarcoidosis
D.
Metastatic disease
E.
Cytomegalovirus (CMV)
Radiologic Findings
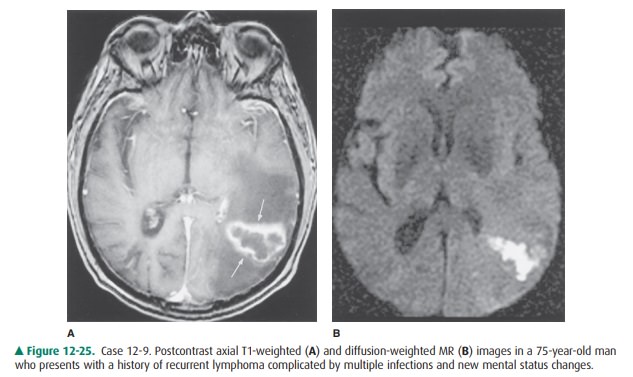
12-9. In this case, the contrast-enhanced MR scan shows a
ring-enhancing lesion (arrows) in the left parietal lobe with decreased
surrounding T1 signal (Figure 12-25 A). A diffusion signal abnormality is
present on the corresponding diffusion-weighted image (Figure 12-25 B), within
the central aspect of the lesion, and is found to be compatible with an area of
restricted water motion. The patient’s history is compatible with an
intracranial infection, and the demonstrated MR imaging findings favor an
abscess (C is the cor-rect answer to Question 12-9.)
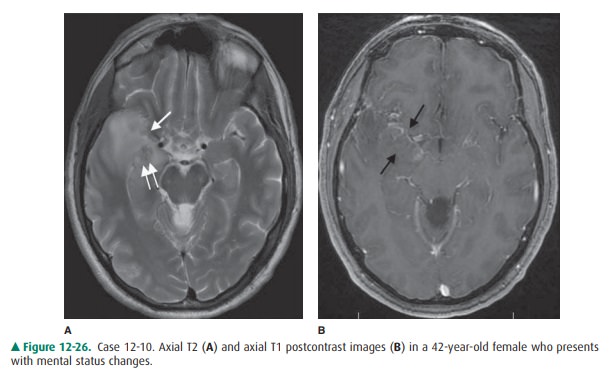
12-10. In this case, the T2-weighted MR image (Figure 12-26shows
increased signal in the medial and anterior aspects of the right temporal lobe
(single arrow) with small focus of T2 hypointensity (double arrows) con-sistent
with the presence of blood products. Postcon-trast axial T1 (Figure 12-26 B)
shows abnormal patchyparenchymal and leptomeningeal enhancement along the
medial right temporal lobe. These changes are commonly seen in patients with
herpes encephalitis (D is the correct answer to Question 12-10).
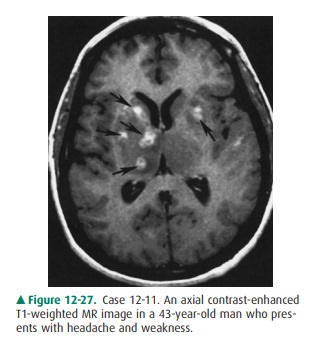
12-11. In this case, multiple enhancing lesions are present
within the basal ganglia, especially on the right (ar-rows), on the
gadolinium-enhanced T1-weighted MR image (Figure 12-27). The most common
lesions with this appearance in an immunocompromised patient, such as a patient
with HIV, are toxoplasmosis and intracranial lymphoma (B is the correct answer
to Question 12-11). The patient markedly improved after anti-toxoplasmosis
therapy, and the lesions shown on the MR image disappeared.
Discussion
A host of infectious diseases can
involve the brain and its cov-erings. Because the CNS has a limited number of
ways of re-sponding to an infectious agent, many intracranial infections appear
identical on neuroimaging studies. It is, therefore, very important to closely
correlate the imaging findings with the clinical presentation and other
diagnostic tests, such as lumbar puncture or stereotactic brain aspiration.
For our purposes, it is useful to
classify CNS infections ac-cording to the intracranial compartment involved,
especially because this has treatment implications. Intracranial infections can
be either parenchymal or extraparenchymal. Parenchymal manifestations include
cerebritis/abscess and encephalitis. Ex-traparenchymal disease includes
epidural abscess, subdural empyema, and leptomeningitis. Bacterial, viral,
fungal, and par-asitic agents can all affect the CNS. Although a few infectious
agents preferentially involve a particular anatomic compart-ment of the CNS,
most are not site specific.
Case 12-9 demonstrates the
classic ring-enhancing lesion of an abscess, in this case, due to Nocardia. No specific fea-tures of this
abscess distinguish it from a typical pyogenic ab-scess. The diffusion signal
abnormality has been postulated to arise from restricted water motion in the
presence of vis-cous, purulent material within the abscess cavity and can mimic
an area of acute ischemia. Cerebral infection by No-cardia usually arises from a pulmonary focus in an
immuno-compromised host. Similarly, most pyogenic abscesses are the result of
hematogenous dissemination from a non-CNS source. Pyogenic brain abscesses can
also result from direct extension of an infectious process from an adjacent
area (eg, sinusitis or mastoiditis) or from trauma (eg, penetrating wound or
surgery).
Abscesses usually occur at gray
matter/white matter junc-tions, although they can occur anywhere in the brain.
Pa-tients frequently present with seizures or symptoms related to intracranial
mass effect. If abscesses develop near the brain surface, they may rupture into
the subarachnoid space, pro-ducing meningitis; they may also produce a
ventriculitis ifthey rupture into the ventricular system. Most abscesses are
treated surgically.
Herpes encephalitis (Case 12-10)
is caused by the herpes simplex virus (HSV). Older children and adults are
usually infected by HSV-1, either primarily or as a result of reactiva-tion of
a latent virus. The ensuing necrotizing encephalitis in this condition
typically involves the temporal and inferior frontal lobes, insular cortex, and
cingulate gyrus. Focal ab-normalities of attenuation (on CT) or signal (on MR)
in these characteristic locations, often with enhancement after contrast
administration, are practically pathognomonic of HSV-1 encephalitis. Early
diagnosis of this condition is ex-tremely important, because antiviral therapy
can signifi-cantly affect patient outcome.
Neonatal herpes simplex infection
differs from infection in the older child and adult. The offending organism is
usu-ally HSV-2, which may be acquired in utero or during birth from mothers
with genital herpes. HSV-2 infection can pro-duce severe destructive changes
within the developing brain. Unlike HSV-1 infection in older children and
adults, neona-tal herpes encephalitis can involve any area of the brain,
hav-ing no predilection for the temporal lobe.
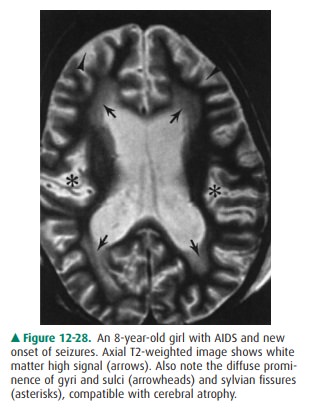
Patients with AIDS (Case 12-11)
commonly develop in-tracranial infections during the course of their disease.
Human immunodeficiency virus (HIV) itself can directly in-fect the CNS,
producing encephalopathy in up to 60% of AIDS patients. The most common
neuroimaging finding in HIV encephalopathy is cerebral atrophy, often with
patchy white matter hypodensity (on CT) or T2 hyperintensity (on MR imaging)
from demyelination and gliosis (Figure 12-28). Other common CNS infections in
the immunocompromised AIDS patient include toxoplasmosis, cryptococcosis, and
progressive multifocal leukoencephalopathy (from a poly-omavirus infection).
Toxoplasmosis usually presents as
multiple lesions of varying size and demonstrates ring enhancement with
sur-rounding edema on CT or MR imaging. Lesions commonly occur in the basal
ganglia or at the gray matter/white matter junction within the cerebral
hemispheres. Individual masses may have a solid appearance or demonstrate
central necrosis or hemorrhage. The enhancement pattern is vari-able; both
rim-enhancing and more solidly enhancing le-sions can be seen. Their appearance
is almost identical to that of primary intracranial lymphoma, another common
intracranial condition in AIDS. Metabolic studies, such as PET or SPECT scans
(no increase in 18F-FDG activity with toxoplasmosis, increased with
lymphoma), MR spec-troscopy (no choline elevation in toxoplasmosis, elevated in
lymphoma), and perfusion-weighted sequences (lower cerebral blood volume in
toxoplasmosis) may assist in dis-tinguishing these pathologies.
Meningitis is the most frequent
manifestation of crypto-coccosis in AIDS, although parenchymal lesions, termed
cryptococcomas, are occasionally encountered. In progressivemultifocal
leukoencephalopathy, extensive areas of white matter demyelination are shown on
MR imaging. A number of other intracranial infections can occur in AIDS
patients.
Related Topics