Chapter: Biology of Disease: Disorders of Water, Electrolytes and Urate Balances
Disorders of Mg2+ Homeostasis
DISORDERS OF Mg2+ HOMEOSTASIS
Magnesium is required to maintain the structures of ribosomes,
nucleic acids and numerous proteins and acts as a cofactor for over 300
enzymes, including those involved in energy metabolism and protein synthesis.
It is also required for normal cell permeability and neuromuscular functions.
The usual dietary intake of Mg2+ is about 15 mmol day–1
and approximately 30% of this is absorbed in the GIT, the rest is lost in the
feces. The adult human body contains over 1200 mmol of Mg2+ (Figure 8.18). Approximately 750 mmol is
found in bone and about 450 mmol in muscle and soft tissues. The ECF contains
only 15 mmol. Approximately 55% of plasma Mg2+ occurs as free
ionized Mg2+, 32% is protein-bound and 13% complexed with Pi
or citrate.
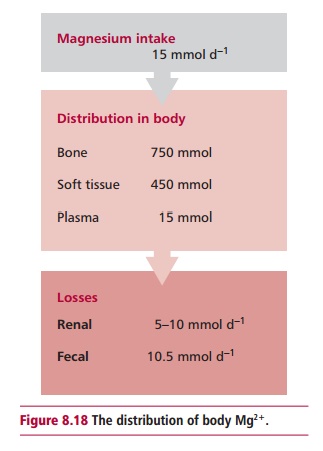
The kidneys lose 5 to10 mmol of Mg2+ daily but losses
are adjusted to control Mg2+ homeostasis. An increased dietary
intake of Mg2+ results in increased renal loss and vice versa. This is achieved principally
by adjusting the reabsorption of Mg2+ by cells of the proximal
tubules and loop of Henle. A number of factors influence the rate of excretion
of Mg2+ including hypercalcemia and hypophosphatemia that decrease
renal reabsorption and PTH, which stimulates renal retention.
The reference range for serum Mg2+ is 0.8–1.2 mmol dm–3.
Hypo- and hypermagnesemia refer to concentrations below and above the reference
range respectively. Note that measurements of the concentration of Mg2+
in plasma or serum are unreliable indicators of its body status since only 1%
of body Mg2+ occurs in the ECF.
The clinical effects of hypomagnesemia are similar to those seen
in hypo-calcemia and include tetany, muscle weakness, convulsions and cardiac
arrhythmias. These effects are related to the role of Mg2+ in
neuromuscular function. The causes of hypomagnesemia include decreased intake
as in starvation , poorly managed parenteral nutrition or malabsorption.
Increased losses of Mg2+ as in osmotic diuresis in diabetics , diuretic
therapy, hyperaldosteronism and excessive losses from the GIT in prolonged
diarrhea, GIT fistula and laxative abuse can also cause hypomagnesemia. The use
of anticancer drugs , such as cisplatinum, can damage the kidneys and prevent
the renal reabsorption of Mg2+. In alcoholism , hypomagnesemia is
believed to occur due to increased renal excretion, inadequate dietary intake,
vomiting and diarrhea.
In many cases, the cause of hypomagnesemia is determined by
clinical examination. However, measuring the urinary Mg2+ may be
useful as the amount of Mg2+ excreted per day decreases with
decreased intake. If hypomagnesemia occurs with increased renal excretion then
losses are likely to be due to renal damage. Hypercalcemia may increase renal
Mg2+ excretion causing hypomagnesemia but hypocalcemia may occur in
hypomagnesemia due to hypoparathyroidism.
In hypomagnesemia, the underlying cause should be treated
wherever possible. Oral Mg2+ supplements may be adequate for mild
cases but severe Mg2+ deficiency together with malabsorption may
require intravenous infusions of Mg2+.
The clinical effects of hypermagnesemia are also largely related
to the role of Mg2+ in neuromuscular activities and include muscular
weakness, respiratory paralysis and, in very severe cases, cardiac arrest.
Acute or chronic renal failures are the commonest causes of hypermagnesemia;
others include its release from damaged cells from, for example, crush
injuries. Mild hypermagnesemia may occur in mineralocorticoid deficiency, as in
Addison’s disease. In rare cases, hypermagnesemia may occur from an increased
oral or parenteral intake of Mg2+ or from the use of Mg2+
containing antacids or laxatives. When this does occur, it is usually combined
with renal failure. The management of hypermagnesemia involves treating the underlying
cause wherever possible. Hypermagnesemia due to renal failure may require
dialysis.
Related Topics