Chapter: Medicine and surgery: Endocrine system
Diabetes mellitus type 1
Diabetes mellitus
Diabetes mellitus type 1
Definition
Type 1 diabetes mellitus is a chronic disorder of carbohy-drate, fat and protein metabolism with hyperglycaemia resulting in most cases from autoimmune destruction of pancreatic ╬▓cells.
Incidence/prevalence
Rare in infancy but rises to 2 per 1000 at age 16. Approximately 10% of all diabetic patients in the UK have Type 1 diabetes.
Age
Any age. Most present aged less than 20 years (peaks at 3ÔÇô4 years and around puberty).
Geography
Wide variation between countries. High in Northern Europe, low in Japan.
Aetiology
Environmentally triggered autoimmune destruction of the pancreatic islet ╬▓-cells in a genetically susceptible individual. There is a concordance of 20ÔÇô40% in monozygotic twins.
Patients have autoantibodies directed against pancreatic islet constituents which may precede the clinical diagnosis by many years.
Polygenic inheritance with Class II MHC associated genes. The IDDM1 major susceptibility gene is involved in familial clustering.
There are specific high risk MHC II haplotypes including HLA-DR3 and -DR4. Having both HLA-DR3 and -DR4 gives an even greater risk than having one or the other. The MHC class II encoded for by these high risk haplotypes is able to present the autoantigen causing lymphocyte activation and hence autoimmune destruction of islet ╬▓-cells. The target autoantigens include glutamate decarboxylase, and insulin. ╬▓-cells may be induced to express MHC Class II by viral infection, which makes the ╬▓-cell present one of its components as an auto-antigen on the cell surface.
Non-MHC related genes are also of importance.
The autoimmune destruction of islet ╬▓-cells is probably triggered by an environmental agent. Type 1 diabetes presents most commonly in autumn and winter, with suggestion of a role for both coxsackie and enteroviruses. Type 1 diabetes is the culmination of an occult process of ╬▓-cell destruction. The autoimmune activity begins up to 10 years before the presentation, which occurs when >95% of the ╬▓-cells have died.
Pathophysiology
The actions of insulin are anabolic (see Fig. 11.14).
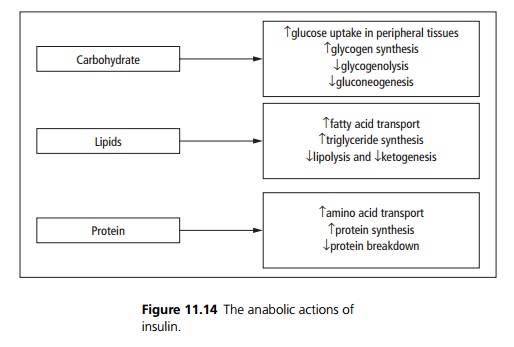
In type 1 diabetes, there is hyperglycaemia due to failure of glucose uptake and uncontrolled gluconeogenesis, glycogenolysis, lipolysis and proteolysis:
┬Ě Osmotic diuresis ÔÇô there is a renal threshold for glucose reabsorption, once the levels in the blood rise above 10 mmol/L the kidney is no longer able to completely reabsorb it from the proximal tubule resulting in glycosuria and an osmotic diuresis.
┬Ě Polydipsia is secondary to the hyperosmolarity and water depletion.
┬Ě Increased appetite occurs.
Clinical features
Patients may present with a history of polyuria, polydipsia and weight loss often despite increased appetite. Young patient often present acutely in diabetic ketoacidosis.
Complications
Acute complications include insulininduced hypoglycaemia and diabetic ketoacidosis.
Chronic complications can be considered as microvascular or macrovascular.
┬Ě Microvascular (microangiopathic) disease includes diabetic retinopathy, diabetic nephropathy and the neuropathies seen in diabetes.
┬Ě Macrovascular (large vessel) disease due to atherosclerosis which leads to complications such as myocardial infarction, strokes, gangrene of the legs and mesenteric artery occlusion.
Investigations
Diagnosis is made on finding symptoms of diabetes (i.e. polyuria, polydipsia and unexplained weight loss) plus one of:
┬Ě A random venous plasma glucose concentration Ôëą11.1 mmol/L or
┬Ě A fasting plasma glucose concentration Ôëą 7.0 mmol/L or
┬Ě A plasma glucose concentration Ôëą11.1 mmol/L 2 hours after 75 g anhydrous glucose in an oral glucose tolerance test (OGTT).
If there are no symptoms diagnosis should not be based on a single glucose determination. Impaired Fasting Glucose (IFG) is defined as a fasting plasma glucose above the normal range but below those diagnostic of diabetes (Ôëą 6.1 mmol/L but <7.0 mmol/L). These patients require an oral glucose tolerance test to exclude diabetes. This is also a risk factor for the future development of diabetes.
Impaired Glucose Tolerance (IGT) is a state of impaired glucose regulation defined as a fasting plasma glucose < 7.0 mmol/L and OGTT two hour value Ôëą 7.8 mmol/L but <11.1 mmol/L). This is a risk factor for the development of diabetes and cardiovascular disease.
Other investigations that may be of value include C-peptide measurement (the cleavage product when proinsulin is converted to insulin) and detection of autoantibodies. These tests are useful in distinguishing patients with type 1 from type 2 diabetes.
Management
Diabetes requires a combination of education, dietary advice, insulin regimens and careful monitoring and follow-up.
Diet: Good nutrition based on a normal proportion of carbohydrate particularly high fibre evenly divided between three main meals. In addition, snacks between meals and at bedtime may be required.
Insulin: It is difficult for subcutaneous insulin therapy to mimic the normal pancreatic secretion into the portal system. Normally the liver immediately takes up 50% of insulin output of the pancreas. Most patients are managed on a twice-daily regimen or basal bolus regimen.
Good control of blood glucose reduces small vessel disease. The Diabetes Control and Complications Trial has shown that only 12% of intensively monitored and treated patients developed retinopathy after 9 years, compared to >50% of the conventionally treated patients.
Monitoring:
Regular capillary blood glucose measurement often premeals, two hours post meals and during the night when changing doses, or at times of instability. Once a patient is stabilised on a particular regimen monitoring may be less frequent.
Glycosylated Hb (HbA1c) is used to assess long-term glycaemic control. It gives an estimate of the average blood glucose over the previous 1ÔÇô2 months.
Patients should be regularly assessed for the development of long-term complications such as nephropa-thy, neuropathy and retinopathy.
Research is continuing into pancreatic and isletcell transplantation. Immunosuppression itself may prevent autoimmune destruction of islet ╬▓-cells and can prevent the development of diabetes in animal models. However there are severe side effects to this treatment.
Related Topics