Chapter: Modern Medical Toxicology: Substance Abuse: Substances of Dependence and Abuse
Designer Drugs - Substances of Dependence and Abuse
Designer Drugs
Designer
drugs are congeners of active compounds that have been modified from legitimate
pharmaceutical agents, and are used for recreational purposes. Apart from
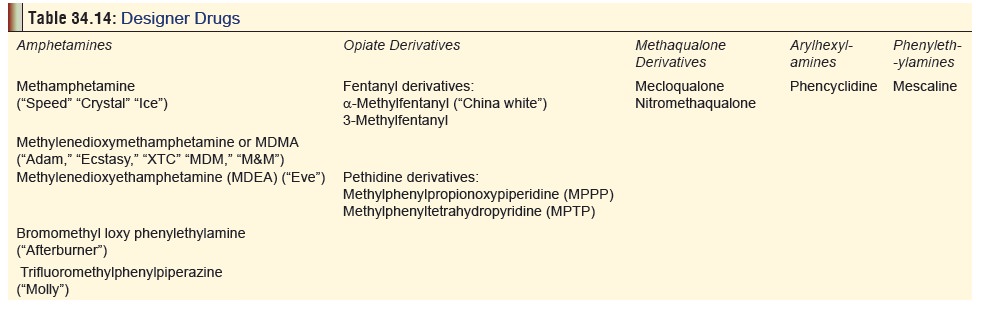
amphetamines, there are several other groups of designer drugs (Table 34.14) which have been discussed
in detail elsewhere.
Designer drugs are usually stronger and cheaper than the
parent compound, and can be easily synthesised in clandestine laboratories. The
term ŌĆ£designer drugŌĆØ does not include new forms or new dosing routes of old
drugs (e.g. cocaine used in freebase form, i.e. ŌĆ£crackŌĆØ). It also does not
include legal drugs which are abused (e.g. ephedrine, caffeine,
phenylpro-panolamine, etc.).
Since
1983 it has become increasingly popular among adolescents and college students
as a recreational drug to be used during ŌĆ£rave partiesŌĆØ which are extended
dance parties often lasting all night long (Fig 34.16). The other designer amphetamines quickly followed and
are mostly available as gelatin capsules or loose powder for ingestion. They
have made their way into India in the late 1990s, and are quite openly abused
by college students from affluent families
Uses
┬Ę
Methylenedioxymethamphetamine (MDMA)
was used in the early years following its synthesis, by psychologists to
enhance psychotherapy. Today, there are no legal uses for any of the designer
amphetamines.
┬Ę
A herbal stimulant (ŌĆśS-5 tabletsŌĆÖ) marketed in the
Netherlands was found to contain para-methylthioamphetamine (p
-MTA or 4-methylthioamphetamine {4-MTA}). It appears to be a potent selective
serotonin releaser without serotonin neurotoxic effects. Efforts are on to make
4-MTA a controlled substance in the United Kingdom under the Misuse of Drugs
Act. The street name for these tablets containing 100 mg of 4-MTA is
ŌĆ£flatlinersŌĆØ.
Mode of Action
┬Ę
While designer amphetamines share a
number of properties with the original amphetamines, unlike the latter, they
are potent releasers of serotonin. Chronic administration can result in
permanent damage to serotonergic neurons. There is strong evidence to suggest
that MDMA use can result in alterations and potential damage to serotonin
neurons. Studies have also indicated that the effects of MDMA on 5-HT neurons
in the human cortex may be reversible in individuals who stop using MDMA, but
the effects of MDMA on memory function may be long-lasting.
Clinical Features
┬Ę
Designer amphetamines are abused by teenagers and young
adults for inducing euphoria, facilitating inti-macy and verbosity, and
heightening sexuality. Users of MDMA report that it ŌĆ£expands consciousnessŌĆØ
without making them lose control. Sometimes these drugs are labelled
ŌĆ£entactogensŌĆØ for their alleged ability to increase sensitivity to touch, or
ŌĆ£empathicogensŌĆØ, for their alleged ability to create empathy, especially before
sexual encounters. MDMA is considered an ŌĆ£entheogenŌĆØ which means ŌĆ£to become
divine from withinŌĆØ. Entheogen refers to a state of shamanic or ecstatic
possession induced by ingestion of mind-altering drugs.
┬Ę
ŌĆ£CandyflippingŌĆØ
refers to the intentional combination of ecstasy with LSD. Another method of
use is called ŌĆ£stackingŌĆØ in which 3
or more tablets of MDMA are taken at once; or MDMA is mixed with alcohol,
cannabis or some other drug (ketamine, GHB, cocaine, etc.) in order to modify
the ŌĆ£highŌĆØ. Stacking can increase the risk of overdose, since MDMA, acting as a
stimulant, can mask the sedative effects of alcohol or any other drug. There is
current vogue for combining ecstasy with sildenafil to enhance sexual pleasure
(ŌĆ£sexstasyŌĆØ).
┬Ę
Acute toxicity results in nausea, anorexia,
anxiety,mydriasis, hyperthermia, muscle rigidity, trismus, sinus tachycardia,
sweating, tachypnoea, cardiac arrhythmias, cardiac arrest, metabolic acidosis,
rhabdomyolysis, myoglobinuria, acute renal failure, and disseminated
intra-vascular coagulation. The following have been reported: convulsions,
cerebral infarcts, hallucinations, paranoia, chest pain, hyperkalaemia, and
fulminant hepatic failure.
┬Ę
Effects are seen 30 to 45 seconds after ingestion (on an
empty stomach) in the form of a ŌĆśrushŌĆÖ, which lasts 15 to 30 minutes. This is
followed by a sense of clarity and joy. A booster dose may be taken at this
point, to prolong these feelings. About ┬Į hour to 3 hours after the initial
ingestion, a ŌĆ£plateauŌĆØ phase occurs in which repetitive or trance-like
movements become extremely pleasurable. The ŌĆ£coming downŌĆØ phase occurs 3 to 6
hours after the initial ingestion, and can lead to negative feelings or
emotions (depression, anxiety). Symptoms may persist for several days.
┬Ę
Hallucinations are common, and may
be auditory or visual in nature. Users often describe seeing trails of lights.
Flashbacks have been reported in several MDMA users. Acute panic attacks and
panic disorder following use of MDMA have also been reported.
┬Ę
Hyperthermia is common in severe
cases, and can contribute to death. It is similar in mechanism to malig-nant
hyperthermia, which is biochemically caused by a rise of calcium ions in the
myoplasm.
┬Ę
Hypertension and tachycardia are
also common, while hypotension and cardiovascular collapse can occur in severe
poisoning.
┬Ę
Cardiac arrhythmias are common in
patients with severe toxicity following MDMA overdose.
┬Ę
Chest pain can occur with ecstasy use combined with physical
exertion. Myocardial infarction has been reported. Spontaneous
pneumomediastinum occurred in another case following the ingestion of three
ecstasy tablets. He also recovered, and was discharged without sequelae.
┬Ę
Pulmonary oedema and ARDS may occur
in severe intoxications.
┬Ę
Convulsions are common in severe
toxicity.
┬Ę
Coma may develop in severe cases.
┬Ę
Intracranial haemorrhages have been
reported with the use of these drugs, as in the case of regular amphetamines
and cocaine.
┬Ę
Acute renal failure has been reported in patients who
develop rhabdomyolysis and/or disseminated intravascular coagulation associated
with MDA, MDEA or MDMA.
┬Ę
Metabolic (lactic) acidosis may occur in severe cases.
Hyperkalaemia and dehydration have been reported. Hypo-natraemia associated
with SIADH has also been reported.
┬Ę
Prolonged INR/PT and PTT, thrombocytopenia, anaemia and
elevated fibrin degradation products have been observed in severe poisonings. A
few cases of aplastic anaemia associated with MDMA use have been reported.
┬Ę
Muscle spasms, jaw clenching, tremors, and hyperre-flexia
are common. Idiopathic temporomandibular joint syndrome (TMJ) has been reported
in some patients, partly due to the secondary effects of bruxism and trismus observed
following acute exposure.
┬Ę
Rhabdomyolysis is a common
complication in patients who develop hyperthermia, seizures, coma, or muscular
hyperactivity.
┬Ę
Eye pain, blurred vision and
diffuse, punctate epithelial erosions of the cornea have been reported in
patients who ingested MDMA and remained awake for long periods of time.
┬Ę
Chronic use results in anorexia, weight loss,
exhaustion,jaundice, irritability, flashbacks, paranoia, depression, or
psychosis. However, since frequent use diminishes the pleasurable effects of
these drugs, users often take them only at intervals of 2 to 3 weeks, and then
gradually lose interest and stop intake altogether over a period of time.*
There appear to be no reports of individuals who take excessive doses of these
drugs frequently over an extended period of time.
┬Ę
There are indications that chronic use of MDMA may cause
mild-to-moderate subclinical impairment in cognitive func-tion, which may be
related to deficits in serotonin (5-HT) function. Chronic paranoid psychosis
has been reported in several cases of individuals chronically abusing MDMA.
┬Ę
Parkinsonian symptoms occurred in some patients following
regular ingestion of MDMA over a prolonged period.
┬Ę
Hepatitis has been reported with chronic abuse.
┬Ę
Ecstasy has been associated with cardiovascular and
musculoskeletal malformations in babies exposed in utero.
Treatment
┬Ę
Treatment measures are essentially
the same as for all ampheta-mine poisonings.
Forensic Issues
┬Ę
Amphetamines are the most widely used illicit drugs (second
only to cannabis) in the United Kingdom, Australia, and many parts of Europe.
Significant abuse also occurs in the USA. After the introduction of
amphetamines into clinical use in the early 1930s, they were available as
prescription drugs for various indications (obesity, narcolepsy, attention
deficit disorder, psychotherapy), and even sold over the counter in the form of
nasal inhalers till the early 1970s. Since then their pharmaceutical use has
been greatly curtailed, though many of these drugs are still available (under
restriction) in Western countries. They are virtually banned in India.
┬Ę
Today, designer amphetamines are a rage among adolescent
party-goers, and are used extensively in the course of ŌĆ£rave partiesŌĆØ. This fad
has now gripped several metropolitan Indian cities where tablets of Ecstasy** (Fig 34.17) are available freely among
elite circles (each tablet costing Rs.300 to 500). Much of this popularity has
to do with the copious amount of informa-tion existing on these drugs on the
Internet, and the fact that unlike certain other drugs like heroin and
cannabis, designer drugs are considered ŌĆ£hepŌĆØ and ŌĆ£coolŌĆØ. Also, unlike many
other
Although
MDMA is classified as a Schedule I drug, it is estimated by the US media that
every year, hundreds of thousands of doses are used illegally. It is most
commonly used by youngsters as they ŌĆ£rollŌĆØ at underground rave parties that can
last for many hours.
Related Topics