Chapter: Modern Medical Toxicology: Substance Abuse: Substances of Dependence and Abuse
Cannabis - Substances of Dependence and Abuse
Cannabis
Source
Cannabis
preparations (vide infra) are derived
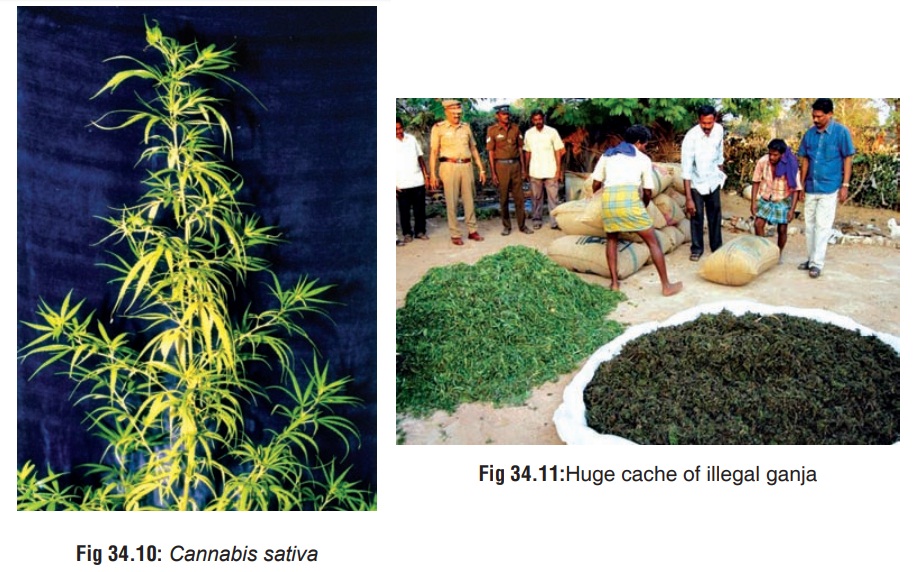
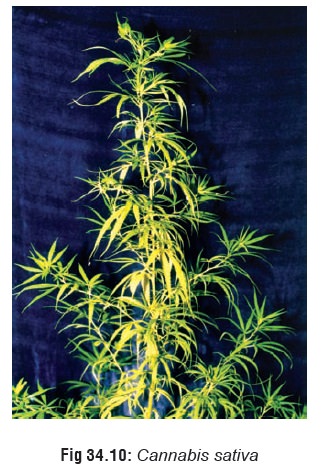
from Indian hemp plant (Cannabis sativa),*
which is a hardy, aromatic annual herb that grows wild under most climatic
conditions (Fig 34.10). The plant
grows to a height of 5 to 15 feet, and is characterised by an odd number of
leaflets on each leaf (varying from 5 to 9), all having serrated or saw-tooth
edges, and small, green flowers. The male and female flowers are borne on
sepa-rate plants. After pollination, the male plants die back.
Active Principles
The main active principle is d9 (delta-9) tetrahydrocannabinol
(THC) which is a cannabinoid found in both the male and female plants. The
concentration of THC is highest in the bracts, flowers, and leaves, while it is
practically non-existent in the stem, root, and seeds. The THC content of the
plant varies greatly, and is probably controlled more by the type of seed than
by the soil or climatic conditions. Depending on the THC content, Cannabis sativa plants are sub-divided
into fibre-type (less than 0.5% THC), or drug-type (more than 1% THC). Seedless
(unpollinated female) plant, referred to as ŌĆ£sinsemillaŌĆØ can contain up to 5%
THC.
THC is a lipid-soluble,
water-insoluble compound which can be synthesised in the laboratory. The
synthetic form, however, is very expensive to produce, and so frequently, other
illicit drugs such as phencyclidine, mescaline, or LSD are sold in the guise of
THC. A product called ŌĆ£super weedŌĆØ or ŌĆ£super grassŌĆØ is dusted with
phencyclidine.
Apart from THC, Cannabis sativa contains a number of other cannabinoids, including cannabidiol, cannabinol, cannabidolic acid, cannabicyclol and cannabigerol.
 Mode of Intake
Mode of Intake
┬Ę
Marijuana: The term ŌĆ£marijuanaŌĆØ refers to any part of the
plant or its extract that is used to induce psychotomimetic or therapeutic effects.
Synonyms include Mary Jane, MJ, maconha, pot, weed, grass, puff, and dagga.
┬Ę
Ganja: Although some texts refer to ganja as being
synonymous with marijuana, while others consider it to be a resinous mass
composed of leaves and bracts, in India (where the term actually originated),
it is used to refer to crushed leaves and inflorescences of female plants (Fig34.11). It is usually smoked in a
pipe (ŌĆ£chillumŌĆØ) or in theform of cigarettes (ŌĆ£reeferŌĆØ or ŌĆ£jointŌĆØ or ŌĆ£numberŌĆØ).
Ganja is said to contain 1 to 2% THC.


┬Ę
Bhang: Bhang consists of dried mature leaves and flower
stems that are ground with water and mixed with milk or fruit juice (Fig 34.12). It is consumed by Hindus in
India during festivals such as Holi and Shiv Ratri.
┬Ę
Hashish (Charas) (Fig
34.13): This preparation is made out of dried resin collected from flower
tops, and contains varying concentrations of THC up to 10%. It is popular in
the Middle East and North Africa. Hashish oil or ŌĆ£liquid hashishŌĆØ is an alcohol
or petrol extract which occurs as a dark green viscous liquid with the
consistency of tar. It is the most potent of all cannabis preparations and
contains 20 to 30% (or more) THC.
┬Ę
Sinsemilla: It is the most popular form of cannabis in the
USA, and refers to seedless (unpollinated female) plant which averages 5% of
THC.
┬Ę
Marijuana ŌĆ£BluntsŌĆØ: This is nothing but cheap cigars sliced
open, packed with cannabis, and resealed. The harsh stench of the cigar masks
the characteristic sweet smell of cannabis. Blunts are very popular among the
youth in some parts of the USA.
Uses
┬Ę
The durable fibres of the woody trunk of cannabis, referred
to collectively as Indian hemp, has been used for centuries to produce rope and
twine, as well as fine or rough cloth. The cannabis plant is possibly the most
efficient source of paper pulp, producing up to 5 times as much cellulose per
acre per year, as trees.
┬Ę
Cannabis seeds are used as food by man, poultry, and other
birds, as well as furnishing hemp-seed oil for paint and soap.
Therapeutic
uses:
┬Ę THC in the form of a synthetic oral cannabinoid (ŌĆ£dron-abinolŌĆØ) has been shown to be effective in controlling the nausea and diarrhoea associated with AIDS, as well as the nausea and vomiting caused by chemotherapy for cancer or AIDS. It also increases appetite and produces weight gain in both AIDS and cancer patients. It is available from Roxane under the trade name Marinol┬«, as round, amber, soft gelatin capsules filled with sesame oil in which either 2.5, 5, or 10 mg of THC is dissolved. Another synthetic cannabinoid, nabilone, is available from Lilly under the trade name Cesamet┬« in the form of 1 mg capsules.
┬Ę
Since smoked cannabis lowers intraocular pressure, it has
been suggested that this effect though short-lived (3 to 4 hours), can be
utilised for treating glaucoma.
┬Ę
Some studies suggest a possible role for cannabis in the
treatment of multiple sclerosis, epilepsy, and dystonic states, though
convincing scientific evidence is lacking.
┬Ę
THC possesses analgesic properties and has been tried in the
treatment of pain due to cancer.
Mode of Action
Recently
a receptor site has been identified in rat brain that binds reversibly and
selectively with cannabinoids. Receptor binding was also found in the
peripheral B lymphocyte-rich areas such as the marginal zone of the spleen,
nodular corona of PeyerŌĆÖs patches, and cortex of lymph nodes. A cannabinoid
antagonist was also discovered that antagonises cannabinoid- induced inhibition
of adenylcyclase and smooth muscle contraction. All this suggests the presence
of a cannabinoid neurochemical pathway. It appears that cannabinoids exert many
of their actions by influencing several neurotransmitter systems and their
modulators. These include GABA, dopa- mine, acetylcholine, histamine,
serotonin, noradrenaline, and prostaglandins.
Cannabinoid
receptor location and density in animal models has correlated well with
clinical effects in humans. The highest density of receptors occurs in the
basal ganglia and molecular layer of cerebellum, which correlates with its
interference in motor co-ordination. Intermediate levels of binding were found
in the hippocampus, dentate gyrus, and layers I and IVof cortex, consistent
with effects on short-term memory andcognition. Low receptor density is noted
in the brainstem areascontrolling cardiovascular and respiratory functions,
whichcorrelates with the cannabinoidsŌĆÖ known lack of lethality.
After
binding to receptors, cannabinoids also produce effects through second-messenger
systems including inhibition of adenylcyclase and calcium channels, and also
probably by enhancing potassium channels activity.
Toxicokinetics
Smoking
cannabis generally produces immediate effects, while ingestion results in slow
and unpredictable effects due to the instability induced by the acidic
environment of the stomach. The most important factor in determining the
bioavailability of THC happens to be the smoking dynamics (manner in which the
cannabis is smoked). It takes about 15 seconds for the lungs to absorb the THC
and transport it to the brain. Peak effects are seen in 10 to 30 minutes and
may last for 1 to 4 hours. The mean terminal half-life of THC in plasma of
frequent cannabis smokers is 4.3 days (range: 2.6ŌĆō12.6 days).
Tetrahydrocannabinol
(THC) is highly protein-bound (97 to 99%), has a Vd of 10 L/kg, and is
enterohepatically recirculated.
THC
is metabolised primarily to 11-hydroxy-delta-9-THC, which is pharmacologically
active, but it is further metabolised to 11-nor-delta-9-THC carboxylic acid,
which is not active.
Clinical Features
1. Acute Poisoning
a. Euphoria with increased garrulity and
hilarity, especially when smoked in a social group setting.
b. Temporal and spatial disorientation with
intensification of sensation (colours become brighter, sounds become more
distinct, music is heard with heightened fidelity) and increased clarity of
perception.
c. At high doses, the user experiences ataxia,
dizziness, hallucinations, sedation, and sometimes dysphoria characterised by unpleasant
sensations, fear, and panic.
d. Sometimes an acute toxic psychosis is
precipitated with suicidal ideation, anxiety, and paranoia. Occasionally,
schizophrenic symptoms occur. Flashback phenomena have been reported.
e.
Tachycardia, palpitations, hypertension (high doses).
Large
doses can also cause postural hypotension.
f.
Stimulation of appetite (especially for sweets).
g.
Reduced bowel motility and urinary retention have occasionally been observed.
h.
Bloodshot eyes due to conjunctival congestion.
i.
Pupils are usually not affected. Occasionally, mydriasis and nystagmus may
occur.
j.
Coma has been reported in children.
2. Chronic Poisoning
┬Ę
Amotivational Syndrome: Chronic
indulgence is said to induce an amotivational syndrome characterised by apathy,
poor concentration, social withdrawal, and lack of motivation to study or work.
However, the actual existence of such a syndrome is being questioned by some
investigators today who state that previous studies had not attempted to
adequately distinguish between the effects of cannabis and pre-existing
psychological status.
┬Ę
In other words, it is difficult to
determine which came first, the drug or the amotivation. Heavy cannabis users
demonstrate an increased tendency to develop manic, schizophreniform, and
confusional psychoses over a period of time. The development of acute psychosis
after chronic use is controversial because of questions about the contribu-
tion of premorbid personalities and multiple-drug use.
┬Ę
Medical complications: Chronic heavy
cannabis use is associated with an increased incidence of the following
conditions:
ŌĆōŌĆō
Chronic lung disease and carcinogenesis: Long-term smoking of cannabis
has been associatedwith chronic sore throat, rhinitis, bronchitis, and
deterioration of pulmonary function suggesting airway narrowing. Experiments
have revealed that cannabis smoking can cause a five-fold increase in blood
CoHb level and three-fold increase in the amount of tar inhaled when compared
with tobacco.
ŌĆōŌĆō
Cancers of mouth and larynx.
ŌĆōŌĆō
Aspergillosis: Studies have shown that cannabis is often contaminated
with Aspergillus spores which can cause aspergillosis in immunocompromised
individuals.
ŌĆōŌĆō
Non-specific ST wave changes have been reported. Prolonged intake of
high doses of THC may result in bradycardia and congestive heart failure.
ŌĆōŌĆō
Several investigators have reported residual poor cognitive performance
in heavy cannabis users, which may be due to alterations in brain function,
residue of the drug present in the brain, or withdrawal effect.
ŌĆōŌĆōDigital clubbing has been reported
in chronic hashish users.
ŌĆōŌĆōGynaecomastia has been observed in
males. Chronic use may also decrease sperm count and fertility.
ŌĆōŌĆō
Abrupt discontinuation of chronic cannabis use can cause a mild
abstinence syndrome consisting of![]() agitation, aggressiveness,
tremulousness, insomnia, sweating, and recurrent migraine headaches.
agitation, aggressiveness,
tremulousness, insomnia, sweating, and recurrent migraine headaches.
Usual Fatal Dose
Ō¢ĀŌ¢Ā There are no
authentically documented cases of lethality from cannabis intoxication alone.
The few cases of fatality that have been reported have not adequately ruled out
the possibility of multiple-drug intoxication.
Ō¢ĀŌ¢Ā In
spite of such lack of documented fatalities, some authors have suggested that
the fatal dose for IV cannabis is about 1 to 2 grams, while it is 700 grams for
ingestion (of bhang).
Ō¢ĀŌ¢Ā According
to some investigators, the estimated lethal dose of cannabis in humans is 30
mg/kg of absorbed cannabis.
Diagnosis
1.
Clinical:
o Symptomatology
o Characteristic ŌĆśburnt ropeŌĆÖ odour in
the breath of a recent smoker.
2. Identification of suspected
specimen: Suspend leaf or stem fragments in several drops of chloral hydrate
(10%) on a microscope slide and examine under low power for characteristic
ŌĆ£cystolith hairsŌĆØ. These hairs look like bear claws or elephant tusks. At the
base of these claws is a wart-like cluster composed of calcium carbonate
deposit. Add a drop of 20% HCl and note the gentle effervescent release of
carbon dioxide gas in tiny bubbles.
3. Urine levels of cannabinoids: THC
is hydrophobic and accumulates in adipose tissue. Screening tests may be
positive for up to 70 or more days, depending on the cut-off levels used and
the individualŌĆÖs lipid stores of THC. False positive results may occur with
therapeutic use of ibuprofen, fenoprofen, and naproxen. False nega-tives may
result from dilution, diuretic use, common salt, or other contaminants
(Visine®*, soap, bleach, vinegar, etc.). Concomitant testing of urine specific
gravity, pH, temperature, and creatinine could help in eliminating these
confounders. Screening tests usually employ EMIT or RIA, while confirmation is
done by using GC-MS. A semiquantitative EMIT homogenous enzyme immuno-assay is
available for measurement of cannabinoids in urine. Hair analysis can detect
drug usage up to 90 days after cessation, and cut-off values are lower for hair
than urine. But it is more expensive, and invariably no more useful than urine
for cannabis detection.
Treatment
Acute Poisoning:
┬Ę
Decontamination measures in cases of
ingestion.
┬Ę
Activated charcoal is beneficial.
┬Ę
Acute psychotic reactions respond to
benzodiazepines.
┬Ę
5 to 10 milligrams of diazepam
orally is usually suffi-cient.
┬Ę
Patients suffering from postural
hypotension should be placed in the Trendelenberg position until the blood
pressure stabilises.
┬Ę
Supportive measures.
Chronic Poisoning:
┬Ę
Psychosocial therapy consisting of
attempts to promote realistic and rewarding alternatives to the drug and
associated life styles, along with a commitment to abstinence from
self-administered or unprescribed psychotropic drugs.
┬Ę
A combination of interventions is
recommended, including urine testing, participation in multi-step programmes,
education about drug effects, drug coun-selling, psychotherapy and family
therapy.
┬Ę
Drug-focussed group therapy
comprising strategies such as social pressure to reinforce abstinence, teaching
socialisation and problem solving skills, reducing stress and the sense of
isolation common with drug abuse, relapse prevention exercises and varying
degrees of confrontation.
┬Ę
Short-term use of anxiolytic agents
such as benzodiaz-epines may be necessary in some cases when anxiety symptoms
are severe.
┬Ę
Short-term use of antipsychotic
medication may be required if there are persistent delusional ideas or
frightening flash backs.
Forensic Issues
┬Ę
Cannabis has been around for thousands of years, initially
touted for its ŌĆ£medicalŌĆØ uses, and later condemned for its abuse potential.
┬Ę
The mind-altering properties of cannabis probably did not
receive wide attention until about 1000 BC when it became an integral part of
Hindu culture in India. After AD 500, cannabis began creeping westward, and
references to it began appearing in Persian and Arabic literature.
┬Ę
Cannabis was brought to Europe by NapoleonŌĆÖs soldiers
returning from Egypt in the early part of 19th century. It made its entry into
the USA at about 1920 when Mexican labourers smuggled the weed across the
border into Texas. Its popularity spread quickly, and by 1937 most of the
American states had enacted laws prohibiting the use or possession of
marijuana. Today, inspite of all efforts at minimising the abuse of cannabis,
the drug is the most commonly used illicit substance in the USA.
┬Ę
The use of cannabis among youth reached its peak in the
1960s when the drug became associated with social protest. The hippie
generation (ŌĆ£flower peopleŌĆØ) was particularly found of cannabis, to whom it was
a ŌĆ£gateway drugŌĆØ opening the doors to more potent ŌĆ£hard drugsŌĆØ such as opiates
and hallucinogens.
┬Ę
Recent reports of medical uses of cannabis have led to the
resurgence of ŌĆ£pot cultureŌĆØ beginning with the 1990s. Consumption of cannabis
in various forms has always been pular in India. Sanyasis and temple poojaris
use it to induce a trance-like state for the purpose of religious medi-tation.
There are several festivals such as Holi and Shiva Ratri when widespread
consumption occurs even among the general populace. In some areas there are
ŌĆ£Bhang shopsŌĆØ openly selling various recipes of bhang (Fig 34.14).
┬Ę
While long-term cannabis use can cause serious health
problems (vide supra), acute
intoxication sometimes leads to medicolegal complications. The danger lies in
the capacity of cannabis to interfere with motor skills and judgement.
Operating a motor vehicle or other machinery under the influ-ence of the drug
could lead to potential loss of life or limb.
┬Ę
Occasional acute psychotic reactions precipitated by long-
term heavy cannabis use can cause the user to ŌĆ£run amokŌĆØ in homicidal frenzy.
This became well known during in homicidal frenzy. This became well known
during suffering from acute toxic psychosis arising out of heavy abuse.
Cannabis is also known to induce suicidal ideation brought on by anxiety and
paranoia.
┬Ę
While cannabis does not appear to have teratogenic effects
on the foetus, some studies have indicated that infants whose mothers had used
the drug during pregnancy exhib- ited impaired foetal growth.
Related Topics