Chapter: Modern Medical Toxicology: Substance Abuse: Substances of Dependence and Abuse
Cocaine - Substances of Dependence and Abuse
Cocaine
Source
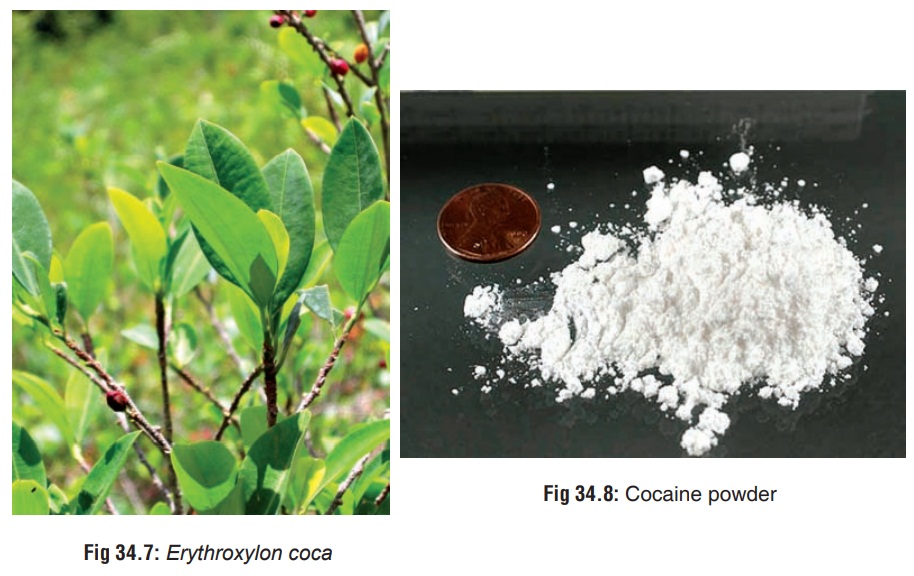
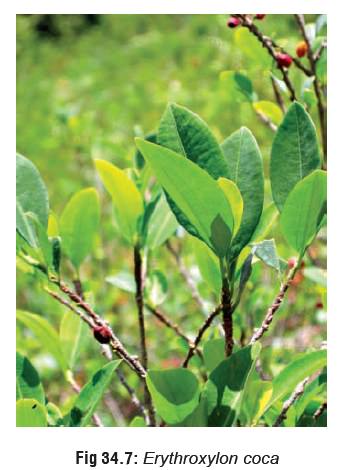
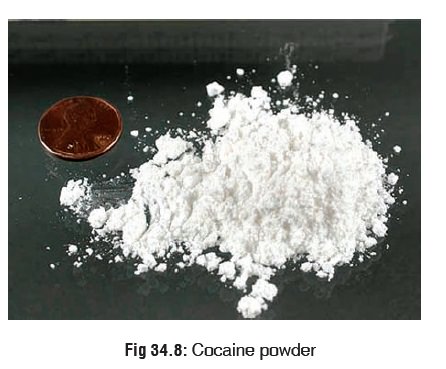
Cocaine (ÔÇťcokeÔÇŁ or ÔÇťsnowÔÇŁ) is a natural alkaloid present in the leaves of the coca plant, i.e., Erythroxylon coca (Fig 34.7), a shrub that grows well in South America, Mexico, Indonesia, and West Indies. Chemically, cocaine is benzoylmethylecgo-nine, and belongs to the tropane family of natural alkaloids, other members of which include atropine and scopolamine. It occurs as colourless to white crystals, or white crystalline powder (Fig 34.8).
Mode of Intake
Cocaine is usually abused by either
chewing coca leaves, smoking coca paste, or ÔÇťsnortingÔÇŁ cocaine hydrochloride. The
last mentioned is the most popular form of cocaine intake, i.e. the drug is
inhaled in powder form through the nostrils. Occasionally, cocaine
hydrochloride is injected intravenously. Today, a smokable form of cocaine (ÔÇťcrackÔÇŁ or ÔÇťrockÔÇŁ) has virtually become a rage in the West. Pure alkaloidal
cocaine (ÔÇťfree-baseÔÇŁ or ÔÇťbaseballÔÇŁ) can also be smoked.
Occasionally coca paste or cocaine sulfate (cocaine base, ÔÇťpastaÔÇŁ, ÔÇťbazookaÔÇŁ) is
smoked. Cocaine freebase is prepared from cocaine hydro-chloride by extracting
the cocaine with an alkaline solution (buffered ammonia) and adding a solvent
such as ether or acetone. The mixture separates into two layers, the top
solvent layer containing the dissolved cocaine. The solvent is then evaporated
leaving almost pure cocaine crystals. ÔÇťFree-baseÔÇŁ
is a colourless, odourless, transparent, crystalline substance that makes a
popping or cracking sound when heated (hence the term ÔÇťcrackÔÇŁ). Both free-base and crack are more stable to pyrolysis than
the hydrochloride salt, and therefore can be smoked either using a ÔÇťcoke pipeÔÇŁ
or mixed into a cigarette (ÔÇťjointÔÇŁ).
A solution of cocaine hydrochloride can also be heated in a pan with baking
soda added until a solid ÔÇťrockÔÇŁ is formed, pieces of which can be smoked
directly.
Street cocaine is often impure. The
content of pure cocaine ranges from 10 to 50 per cent (most commonly 15 to 20
per cent). Cocaine which is available on the street is often adul-terated with
one or more of the following compounds: talc, lactose, sucrose, glucose, mannitol,
inositol, caffeine, procaine, phencyclidine, lignocaine, strychnine,
amphetamine, or heroin (ÔÇťspeed ballÔÇŁ).
Crack cocaine adulterated with phenytoin (in order to lower cost or increase
potency) has resulted in pheny-toin toxicity in some patients.
Uses
ÔľáÔľá Topical anaesthetic
(4 to 10% solution) for intranasal and bronchoscopic procedures.
ÔľáÔľá Ophthalmologic
anaesthesia.
ÔľáÔľá Relief of severe
(oncologic) pain: Cocaine is one compo-nent of BromptonÔÇÖs cocktail, (the others
being morphine, chlorpromazine, and alcohol), which is popular in Europe for
the control of intractable pain associated with some forms of cancer.
ÔľáÔľá Cocaine is one of
the components of TAC (the others being tetracaine and adrenaline) which is
sometimes used as a topical anaesthetic in children with scalp and facial
lacerations.
Mode of Action
CNS:
o Cocaine is the most powerful
naturally derived CNS stimulant known to man. Stimulation of the brain occurs
in a rostral-to-caudal fashion. The cortex is stimulated first resulting in
excitement, restlessness, and increased motor activity. Subsequent stimulation
of lower motor centres produces tonic-clonic convulsions. The medulla is at
first stimulated resulting in an initial increased respiratory rate, followed
by depression with resultant respiratory failure.
o The CNS stimulant effects of cocaine
are mediated through inhibition of dopamine reuptake in the nucleus accumbens.
A recent study affirms the central importance of the dopamine-reuptake
transporter in the behavioural and biochemical action of cocaine and defines it
as a site on which efforts to develop an anti-cocaine medication should be
focused. The dopamine-reuptake transporter controls the levels of dopamine in
the synapse by rapidly carrying the neurotransmitter back into nerve terminals
after its release. Cocaine, which binds strongly to the dopamine-reuptake
transporter, is a classic blocker of such reuptake after normal neuronal
activity. Because of this blocking effect, dopamine remains at high
concentrations in the synapse and continues to affect adjacent neurons
producing the characteristic cocaine ÔÇťhighÔÇŁ.![]()
o Cocaine also increases the
concentrations of the excitatory amino acids, aspartate and glutamate in the
nucleus accumbens. These excitatory amino acids increase the extracellular
concentrations of dopamine. Excitatory amino acid antagonists attenuate the
effects of cocaine induced convulsions and death. Dopamine2 (D2)
receptor agonists accentuate cocaine craving, while dopmanie1 (D1)
agonists diminish such craving.
o Cocaine also inhibits reuptake of
noradrenaline and serotonin. Increase in the concentrations of the former plays
an important role in the toxic effects of cocaine.
Peripheral nerves: Through direct
blockade of fast sodium channels, cocaine stabilises the axonal membrane,
producing a local anaesthetic effect. Cocaine is the only local anaesthetic
that interferes with the uptake of neuro-transmitter by the nerve terminals and
simultaneously functions as a vasoconstrictor.
CVS:
o Initial effect of cocaine on the CVS
is bradycardia, secondary to stimulation of vagal nuclei. However, the
bradycardia is too transient to be clinically evident, and tachycardia becomes
the prominent effect resulting from central sympathetic stimulation.
o Cocaine produces blockade of fast
sodium channels on myocardial tissue, imparting type I antiarrhythmic
properties. The cardiostimulatory effect of cocaine is due in large part to
sensitisation to adrenaline and noradrenaline, preventing neuronal reuptake of
these catecholamines, as well as due to increased release of noradrenaline from
adrenergic nerve terminals. The increased concentrations and persistence of
catechola-mines near the receptors of the effector organ lead to exaggerated
sympathetic effects.
o Studies have revealed that the peak
vasopressor effects of cocaine are mediated by noradrenaline of sympa-thetic
neural origin, while the peak tachycardic effects are mediated by direct
release of adrenaline of adrenal medullary origin.
o The sympathomimetic effects of
cocaine increase myocardial oxygen demand and the alpha-adrenergic mediated
coronary vasoconstriction limits coronary artery blood flow. Cocaine inhibits
endogenous fibrinol-ysis, increases thrombogenicity, and enhances platelet
aggregation.
Toxicokinetics
AbsorptionÔÇö
┬Ě
Ingestion and insufflation: Cocaine
is well absorbed from oral, nasal, and pulmonary routes. Onset of action on
insufflation is within 1 to 3 minutes, and peak effects are seen in 20 to 30
minutes.
┬Ě
Intravenous injection: Onset of
action is within seconds, and peak action occurs in 3 to 5 minutes.
┬Ě Inhalation: Smoking produces effects as rapidly as IV injection.
MetabolismÔÇö
┬Ě
Cocaine is metabolised by liver
esterases and plasma cholinesterase to ecgonine methylester (EME), one of the
major metabolites, while non-enzymatic hydrolysis results in the formation of
the other major metabolite, benzoylecgonine (BE). Minor metabolites include
norcocaine ecgonine, ecgonidine, norecgonidine methylester, norecgonine
methylester, and m-hydroxy- benzoylecgonine.
ExcretionÔÇö
┬Ě
The biologic half-life of cocaine is
┬Ż to 1┬Ż hours.
┬Ě
Benzoylecgonine and ecgonine
methylester possess half lives of 5 to 8, and 3┬Ż to 6 hours respectively.
Excretion is mainly through urine. Due to the long elimination half-life of BE,
assays for its detection in urine may be successful up to 2 to 3 days following
cocaine use. In rare cases, it has been detected even after 22 days.
Clinical Features
Acute Poisoning
a.
HyperthermiaÔÇöThis results from
ÔÇôÔÇô
Augmentation of heat production due to increased psychomotor activity.
ÔÇôÔÇô
Diminution of heat dissipation due to vasoconstric-tion.
ÔÇôÔÇô
Direct pyrogenic effect due to action on thermoreg-ulatory centres in the
hypothalamus.
ÔÇôÔÇô Stimulation of calorigenic activity of liver.
b.
Body temperature often soars to 108┬░ to 112┬░F, and does not respond to
conventional antipyretics. It is often associated with rhabdomyolysis,
seizures, and renal
failure.
ÔÇôÔÇô
CNS effectsÔÇö -- Headache:
┬╗┬╗ Pattern 1ÔÇöDevelops within minutes, andlasts for 2 to 48 hours. The
headache is usually occipital or bilateral, with associ-ated throbbing,
photophobia, nausea, and vomiting.
┬╗┬╗ Pattern 2ÔÇöOccurs during a cocaine ÔÇťbingeÔÇŁ,(4 to 14 days of abuse, 1
to 3 g/day), with onset after a few days, which increases in severity
progressively. It is mostly frontal, with associated throbbing, nausea and
some-times diplopia and dizziness.
┬╗┬╗ Pattern 3ÔÇöOccurs 1 to 4 days after the lastdose of cocaine, and
worsens over the next 1 week with continued abstinence. It is also frontal,
with associated throbbing, nausea, vomiting, photophobia, and occasionally neck
stiffness.
ÔÇôÔÇô
Anxiety, agitation.
ÔÇôÔÇô Hyperactivity, restlessness. ÔÇôÔÇô
Tremor, hyperreflexia.
ÔÇôÔÇô Convulsions: Generalised
tonic-clonic, partial motor, and partial complex seizure have all been
reported. Seizures may be recurrent and status epilepticus has been reported,
particularly in chil-dren. Sometimes there is lethargy and decreased level of
consciousness which can persist up to 24 hours (ÔÇťcocaine washed out syndromeÔÇŁ).
ÔÇôÔÇô Cerebrovascular accidents are not
uncommon, and include subarachnoid haemorrhage, intrac-erebral haemorrhage,
cerebral infarction, tran-sient ischaemic attacks, migraine-type headache
syndrome, cerebral vasculitis, and anterior spinal artery syndrome. Infarction
of the brainstem/spinal cord has occurred.
c. Psychiatric effectsÔÇö
ÔÇôÔÇô Paranoid state with
suspiciousness, hypervigilance, anxiety.
ÔÇôÔÇô
Stereotypy.
ÔÇôÔÇô Hallucinations. ÔÇôÔÇô Toxic
delirium.
d. Ophthalmologic effectsÔÇö
ÔÇôÔÇô Mydriasis and/or loss of eyebrow
and eyelash hair from smoking crack cocaine may occur.
ÔÇôÔÇô Corneal abrasions/ulcerations due
to particulate matter in smoke (ÔÇťcrack
eyeÔÇŁ).
ÔÇôÔÇô Central retinal artery occlusion
and bilateral blind-ness due to diffuse vasospasm. Retinal foreign body
granuloma may occur with IV abuse.
e. CVS effectsÔÇö ÔÇôÔÇô Tachycardia.
ÔÇôÔÇô
Systemic arterial hypertension.
ÔÇôÔÇô Coronary artery vasoconstriction
with myocardial ischaemia and infarction. Coronary artery disease, heavy
smoking, and hypertension are predisposing factors. Myocardial infarction may
occur even in young patients without risk factors or pre-existing cardiac
pathology.
ÔÇôÔÇô Tachyarrhythmias of all types can
occur, including sinus tachycardia, atrial fibrillation or flutter, other
supraventricular tachycardias, ventricular premature contractions, ventricular
tachycardia, torsades de pointes, and ventricular fibrillation. Sinus
tachy-cardia is the most common finding. If hypertension is significant, a
reflex bradycardia may occur. Cocaine-induced syncope and bradyarrhythmia have
been reported in some cases.
ÔÇôÔÇô Chronic dilated cardiomyopathy
can occur.
ÔÇôÔÇô Aortic dissection and rupture.
f. Pulmonary effectsÔÇö
ÔÇôÔÇô Thermal injuries to the upper
airway leading to epiglottitis, laryngeal injury, and mucosal necrosis have
been reported after smoking ÔÇťcrackÔÇŁ or free base cocaine.
ÔÇôÔÇôExacerbation of asthma.
ÔÇôÔÇô
Noncardiogenic pulmonary oedema is a common finding at autopsy.
ÔÇôÔÇô Pneumothorax, pneumomediastinum.
ÔÇôÔÇôDiffuse alveolar haemorrhage.
ÔÇôÔÇô
Bronchiolitis obliterans with organising pneumonia.
g. Musculoskeletal
effectsÔÇöRhabdomyolysis with hyper- thermia, massive elevation of creatine
phosphokinase, and acute renal failure. Although the mechanism of
cocaine-associated rhabdomyolysis is unclear, it is postulated that it may
result from ischaemia due to vaso- constriction, direct toxicity, hyperpyrexia,
and increased muscle activity from agitation or seizure activity.
h. GI effectsÔÇö
ÔÇôÔÇôAcute mucosal ischaemia.
ÔÇôÔÇôColitis.
ÔÇôÔÇô
Intestinal perforation: It is postulated that cocaine blocks the
reuptake of noradrenaline leading to mesenteric vasoconstriction and focal
tissue ischaemia and perforation.
ÔÇôÔÇô
Pneumoperitoneum has been reported after smoking crack cocaine.
ÔÇôÔÇô Hepatic
necrosis (centrilobular, midzonal, and panlobar) has been reported in overdose.
R
i. enal effectsÔÇöRenal failure, usually
secondary to myoglobinuria and rhabdomyolysis, has been reported after
intravenous or intranasal cocaine use. Renal infarc- tion has occurred
following intravenous cocaine use.
j. Uteroplacental effectsÔÇö
ÔÇôÔÇô
Increased incidence of spontaneous abortion, low birthweight, and
abruptio placentae. Neonatal intoxi- cation may also occur. Infants exposed to
cocaine in utero may display tremulousness, impaired orienta- tion, increased
startle response, irritability, muscular rigidity, arousal deficits, impaired
motor ability, and lower scores on the Brazelton Neonatal Behavioural
Assessment Scale (measuring interactive behaviour and response to environmental
stimuli).
ÔÇôÔÇô
There are indications that cocaine may be terato- genic.
ÔÇôÔÇô Cocaine
toxicity has been reported in breastfed infants of cocaine abusing mothers.
k. Miscellaneous effectsÔÇö
ÔÇôÔÇô
Priapism has been observed after topical applicationof cocaine to the
glans penis.
ÔÇôÔÇô
Severe metabolic acidosis has been reported due to seizures, agitation,
and hypotension.
l. Drug combination effectsÔÇö
ÔÇôÔÇô Cocaine is often combined with
other drugs such as ethanol and heroin. Concurrent use of cocaine and ethanol
produces additive effects on the brain. It results in the formation of the
metabolite, cocaeth-ylene which is more cardiotoxic, and is associated with
enhanced mortality.
ÔÇôÔÇôCombination of cocaine with heroin
is referred to as ÔÇťspeed ballÔÇŁ and is
reputed to produce a double effect of initial high ÔÇťkickÔÇŁ of cocaine, followed
by subsequent euphoric ÔÇťrushÔÇŁ of heroin. ÔÇťSpeed
ballÔÇŁ is usually injected.![]()
Chronic Poisoning
a. Cocaine dependence
ÔÇôÔÇô Cocaine dependence is defined in
DSM-IV as a cluster of physiological, behavioural, and cognitive symptoms that,
taken together, indicate that the person continues to use cocaine despite
significant problems related to such use.
ÔÇôÔÇô Some cocaine users can use
cocaine intermittently without becoming dependant, though it is not clear how
long such intermittent, non-dependant use can continue. Intermittent use
consists of episodes or binges of use, often starting on weekends and paydays,
and lasting until the drug supply is exhausted or toxicity develops. Such
binges, during which the drug may be used every 15 to 30 minutes, can last 7 or
more consecutive days (though usually this extends to only 3 or 4 days). When
the binge comes to an end, a ÔÇťcocaine
crashÔÇŁ occurs.
b. Cocaine abuse
ÔÇôÔÇô Some cocaine abusers develop
problems or adverse effects related to their drug use (i.e. their use is
mala-daptive). Examples of such recurrent maladaptive patterns include use that
leads to multiple legal prob-lems, failure to meet major social, school, or
work-related obligations, and continued use despite social or vocational
difficulties caused by, or aggravated by cocaine use. When one or more such substance-related
problems occur in a 12-month period, the diagnosis of cocaine abuse is made.
ÔÇôÔÇô Chronic use of cocaine leads to
CNS dopamine depletion and increases in the number and sensi-tivity of dopamine
receptors. The dysphoric state associated with cocaine withdrawal (vide infra) and craving for cocaine
appears to be a result of the dopamine-depleted condition.
ÔÇôÔÇô Features of chronic cocaine use:
-- Anorexia, emaciation.
--
Mydriasis.
-- Agitation, restlessness: A
cocaine-associated agitated delirium
syndrome has been identified,comprising the following in sequence:
hyper-thermia, delirium with agitation, respiratory arrest and death.
-- Hallucinations, especially
tactile, characterised by a crawling sensation under the skin (ÔÇťcocainebugsÔÇŁ) with resultant
excoriation, leading toirregular scratches and ulcers (MagnanÔÇÖs sign).
Perceptual disturbances or pseudo-hallucinations involving vision (ÔÇťsnow
lightsÔÇŁ, geometric patterns), smell, hearing and taste have also been reported.
--
Tremor.
-- Recurrent chest pain. --
Cardiomyopathy.
--
Psychiatric changes: depression, psychosis, panic disorders, attention deficit
disorders, and eating disorders.
--Decreased libido, impotence,
gynaecomastia, galactorrhoea, amenorrhoea, and sexual dysfunction are common with
chronic cocaine abuse.
--Cocaine abuse may be associated
with cerebral atrophy.
--ÔÇťCrack handsÔÇŁ: A syndrome of multiple, black-ened, hyperkeratotic lesions (linear or circular), of the fingers and palms has been described in crack cocaine smokers. These lesions probably result from the heat of the glass cocaine pipe.
--Maternal chronic cocaine use
during preg-nancy has been suggested as a possible factor in Sudden Infant
Death Syndrome. Cocaine readily passes into breast milk and can cause adverse
effects in the nursing infant.
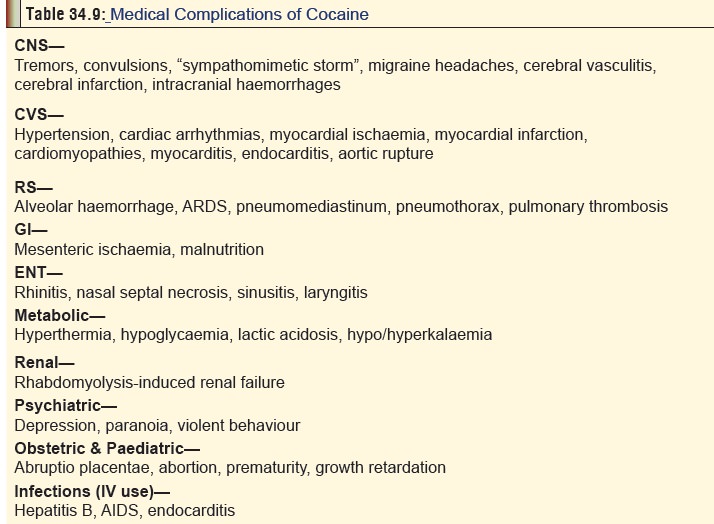
--Evidence of medical complications
(Table34.9).
c. Cocaine withdrawal
ÔÇôÔÇô Conventionally, cocaine
withdrawal is said to occur in 3 phases:
Phase I (ÔÇťCrashÔÇŁ): The total duration of this phaselasts for
anywhere between 9 hours and 4 days, and is subdivided further into the
following stagesÔÇö
┬╗┬╗Early: Agitation depression,
anorexia, intense craving for cocaine.
┬╗┬╗Intermediate: Fatigue, tendency to
sleep, decreased craving.
┬╗┬╗Late: Exhaustion, hypersomnia,
hyperphagia, absence of craving.
Phase II: Normalised sleep, improved mood, followedsubsequently by
return of anergia, anhedonia, anxiety, and increased craving.
Phase III: (ÔÇťExtinctionÔÇŁ): Increased tendency to relapse.The
extinction phase may be prolonged and consists of brief, episodically evoked
cravings that occur months to years after withdrawal.
ÔÇôÔÇô
Additional points of importance:
-- Impaired colour vision
(blue-yellow), which may persist for up to 2 months or more, has been reported
in some patients with cocaine with-drawal. A dysregulation of blue cone
function has been suggested, since significantly reduced blue cone
electroretinogram responses have been observed in recently withdrawn
cocaine-dependant patients.
-- Silent ischaemia has occurred
upon cocaine withdrawal, and acute myocardial infarction may occur up to 2
weeks after the last cocaine use.
-- ECG changes: Increased PR
intervals have been found to correlate with length of abstinence, which is
thought to reflect the remediation of a depolarisation variant. Chronic cocaine
users may be subject to rapid cardiac depolarisation (decreased PR intervals)
that gradually returns to normal over 20ÔÇô30 days.
-- EEG changes: Evaluation of quantitative EEGs in cocaine-dependant persons after a 10-day drug free interval revealed increased power in the beta-2 band that correlated with the frequency of cocaine use during the last 30 days before hospital admission. Elevated power of EEG beta (fast EEG activity) could be a neurophysiological cocaine withdrawal sign.
--Persistently elevated serum
creatine kinase (CPK) levels (>374 Units/L) have been demon-strated in
abstinent cocaine abusers, with evidence of impaired spatial motor
perfor-mance, and tendency to coarse motor control and impulsive movements.
--Withdrawal from cocaine sometimes
results in hyperprolactinaemia during the first month, which may be due to its
effect on serotonergic function. Bromocriptine (0.625 mg orally, twice daily)
may be of value for treating cocaine withdrawal-induced hyperprolactinaemia.
--Cocaine readily crosses the
placental barrier, causing an alteration of the central neurotrans-mitter
state, and increasing peripheral catechola-mines in the foetal circulation. In
utero cocaine exposure in a foetus nearing term could result in altered
behaviour after delivery, consistent with drug abstinence, and in decreased
flow velocity in the anterior cerebral artery consistent with the
vasoconstrictive effects of cocaine. Abstinence symptoms are seen in the first
and second postnatal days, and may last for several weeks. Cocaine-exposed
infants may be at an increased risk for sudden infant death syndrome (SIDS).
Symptoms of neonatal cocaine abstinence syndrome include irritability,
hypertonia/poor muscle tone, tremor, hyperactive Moro reflex, loose stools,
sleep disturbances, poor feeding/ excessive sucking, nasal stuffiness,
tachypnoea, visual function disturbance.
Usual Fatal Dose
ÔľáÔľá About
500 mg (oral).
ÔľáÔľá About 100 mg (mucosal contact).
ÔľáÔľá Lethal
blood level: 0.2 mg/100 ml.
Chronic
users of cocaine can tolerate much higher doses.
Related Topics