Chapter: Medical Surgical Nursing: Management of Patients With Musculoskeletal Trauma
Clavicle - Fracture
Fractures
of Specific Sites
Injuries to the skeletal
structure may vary from a simple linear fracture to a severe crushing injury.
The type and location of the fracture and the extent of damage to surrounding
structures deter-mine the therapeutic management. Maximum functional recov-ery
is the goal of management.
CLAVICLE
Fracture of the clavicle
(collar bone) is a common injury that re-sults from a direct blow to the
shoulder or a fall. Head or cervical spine injuries may occur with these
fractures. The clavicle helps to hold the shoulder upward, outward, and
backward from the thorax. Therefore, when the clavicle is fractured, the
patient as-sumes a protective position, slumping the shoulders and
immo-bilizing the arm to prevent shoulder movements. The treatment goal is to
align the shoulder in its normal position by means of closed reduction and
immobilization.
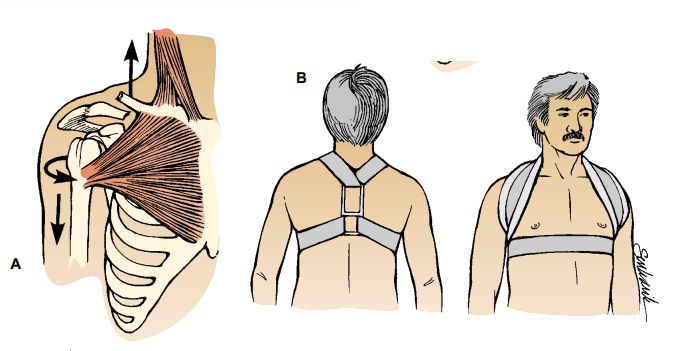
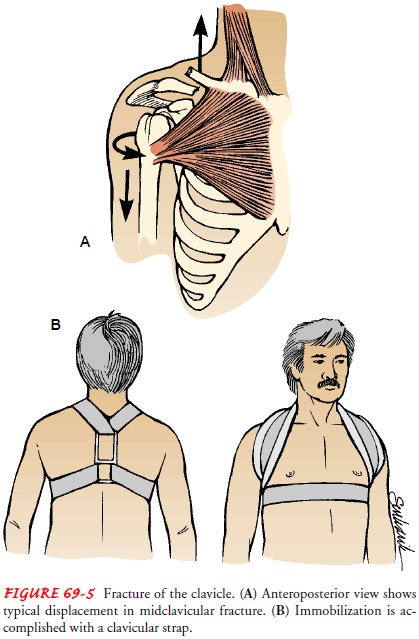
More than 80% of these
fractures occur in the middle third of the clavicle. A clavicular strap, also
called a figure-of-eight bandage (Fig.
69-5), may be used to pull the shoulders back, reducing and immobilizing the
fracture. When a clavicular strap is used, the axillae are well padded to
prevent a compression injury to the brachial plexus and the axillary artery.
The nurse monitors the cir-culation and nerve function of both arms. A sling
may be used to support the arm and to relieve pain. The patient may be
permit-ted to use the arm for light activities within the range of comfort.
Fracture of the distal
third of the clavicle, without displacement and ligament disruption, is treated
with a sling and restricted mo-tion of the arm. When a fracture in the distal
third is accompanied by a disruption of the coracoclavicular ligament, there is
displace-ment, which may be treated by open reduction and internal fixation.
Complications of clavicular fractures include trauma to the nerves of the brachial plexus, injury to the subclavian vein or artery from a bony fragment, and malunion (poorly aligned healing of the fractured bone). Malunion may be a cosmetic problem (eg, when low-neckline clothing is worn).
Nursing Management
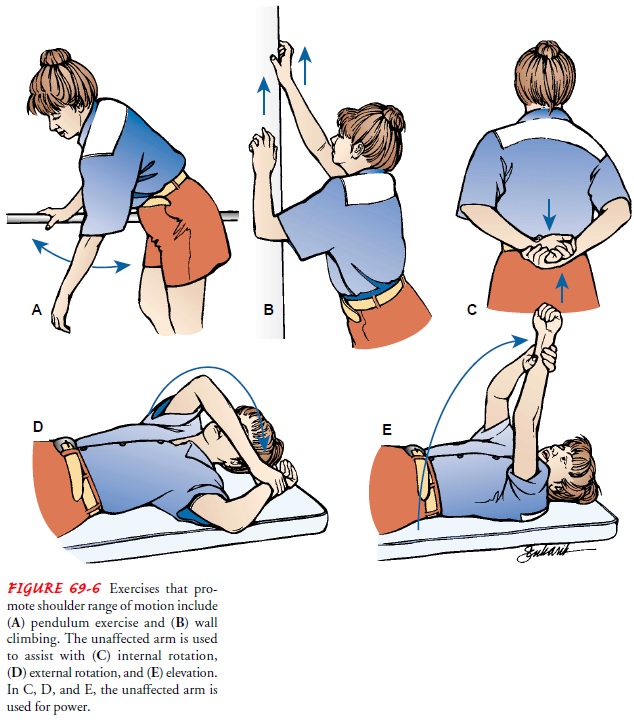
The nurse cautions the patient not to elevate the arm
above shoul-der level until the ends of the bone have united (about 6 weeks)
but encourages the patient to exercise the elbow, wrist, and fingers as soon as
possible. When prescribed, shoulder exercises (Fig. 69-6) are performed to
obtain full shoulder motion. Vigorous activity is limited for 3 months.
Related Topics