Chapter: Ophthalmology: Glaucoma
Childhood Glaucomas
Childhood Glaucomas
Definition
Any abnormal increase in intraocular pressure during
the first years of life will cause dilatation of the wall of the globe, and
especially of the cornea. The result is a characteristic, abnormally large eye
(buphthalmos) with a progress-ive increase in corneal diameter. This is also
referred to as hydrophthalmos or hydrophthalmia.
Epidemiology:
Glaucomas in children occur once every 12000 – 18000births and
account for about 1% of all glaucomas. Primary congenital glau-coma is an
inherited autosomal recessive disorder. It is bilateral in approxi-mately 70%
of all cases; boys are affected in approximately 70% of all cases; and glaucoma
manifests itself before the age of six months in approximately 70% of all
cases.
Today there is widespread public awareness of
glaucoma in adults.
Unfortunately, this does not yet apply to
glaucoma in children.
Etiology:
(See also physiology and pathophysiology of aqueous humor
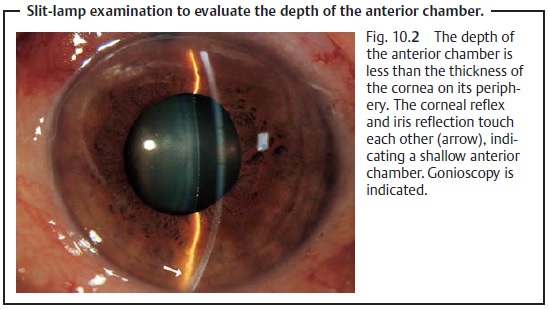
circu-lation): The iris inserts anteriorly far in the trabecular meshwork (Fig.
10.2). Embryonic mesodermal tissue
in the form of a thin transparent membrane (Barkan’s membrane) covers the
trabecular meshwork and impedes the flow of aqueous humor into the canal of
Schlemm. Other abnormal ocular or systemic findings are lacking.
Aside from isolated buphthalmos, other ocular
changes can lead to sec-ondary hydrophthalmos. These include:
❖ Hydrophthalmia with ocular developmental
anomalies.❖ Hydrophthalmia with systemic disease.
❖ Secondary buphthalmos resulting from acquired
eye disorders.
Regardless of the cause of the increase in
intraocular pressure, the objective signs and clinical symptoms of childhood
forms of glaucoma are identical and should be apparent to any examining
physician.
Symptoms:
Classic signs include photophobia, epiphora, corneal
opacifica-tion, and unilateral or bilateral enlargement of the cornea. These
changes may be present from birth (in congenital glaucoma) or may develop
shortly after birth or during the first few years of life.
Children with this disorder are irritable,
poor eaters, and rub their eyes often. The behavior of some children may lead
one to suspect mental retarda-tion.
Physicians should be alert to parents who
boast about their child’s “big beautiful eyes” and should measure intraocular
pressure.
It is essential to diagnose the disorder as
early in the child’s life as possible to minimize the risk of loss of or
irreparable damage to the child’s vision.
Diagnostic considerations:
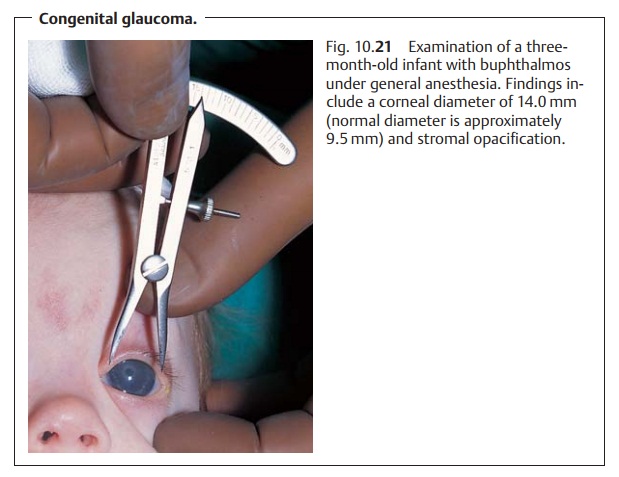
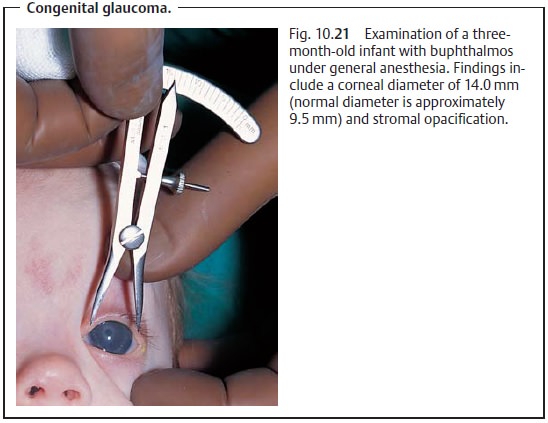
These examinations may be performed withoutgeneral anesthesia in many children. However, general anesthesia will occa-sionally be necessary to confirm the diagnosis especially in older children (Fig. 10.21).
Measurement of intraocular pressure.One should generally attempt tomeasure intraocular pressure by applanation
tonometry (tonometry with a hand-held tonometer).
Measurement is facilitated by giving the
hungry infant a bottle during the examination. Feeding distracts the baby, and
a measurement usu-ally can be obtained easily. Such a measurement is usually
far more accurate than one obtained under general anesthesia as narcotics,
especially barbiturates and halothane, reduce intraocular pressure.
Optic disk ophthalmoscopy.The optic cup is a very sensitive indicator ofintraocular
pressure, particularly in the phase in which permanent visual field defects
occurs. Asymmetry in the optic cup can be helpful in diagnosing the disorder
and in follow-up.
Special considerations: A glaucomatous optic cup in children may well bereversible.
Often it will be significantly smaller within several hours of a successful
trabeculotomy.
Inspection of the cornea.The cornea will appear whitish and opacified due toepithelial
edema. Breaks in Descemet’s membrane can exacerbate an epithelial or stromal
edema. These lesions, known as Haab’s striae, will exhibit a typical horizontal
or curvilinear configuration.
The enlarged corneal diameter is a
characteristic finding. The cornea nor-mally measures 9.5 mm on average in
normal newborn infants. Enlargement to more than 10.5 mm suggests childhood
glaucoma. Chronically elevated intraocular pressure in children under the age
of three will lead to enlarge-ment of the entire globe.
Gonioscopy of the angle of the anterior chamber.Examination of the angleof the anterior
chamber provides crucial etiologic information. The angle will not be fully
differentiated. Embryonic tissue will be seen to occlude the trabecular
meshwork.
Differential diagnosis:
Large eyes.A large corneal diameter can occur as
aharmless anomaly (megalocornea).
Corneal opacification.Diffuse corneal opacification with epithelial edemaoccurs in
congenital hereditary endothelial dystrophy. Opacification with-out epithelial
edema occurs in mucopolysaccharidosis (Hurler’s syn-drome, Scheie’s syndrome,
Morquio’s syndrome, and Maroteaux-Lamy syn-drome).
Striae in Descemet’s
membrane.In contrast to the
horizontal Haab’s striae incongenital glaucoma, endothelial breaks can also
occur as a result of injury during a forceps delivery (vertical striae), in
keratoconus, and in deep ker-atitis.
None of these differential diagnoses are
accompanied by elevated intraocular pressure.
Treatment: Childhood glaucomas are treated surgically. The
prognosisimproves the earlier surgery is performed.
Principle and procedure of goniotomy.With a gonioscope in place on theeye, the
goniotomy scalpel is advanced through the anterior chamber to the trabecular
meshwork. The trabecular meshwork can now be incised as far the canal of
Schlemm over an arc of about 120 degrees to permit drainage of the aqueous humor.
Often two or three goniotomies at different locations are required to control
intraocular pressure. These operations can only be per-formed when the cornea
is clear enough to allow visualization of the struc-tures of the anterior
chamber.
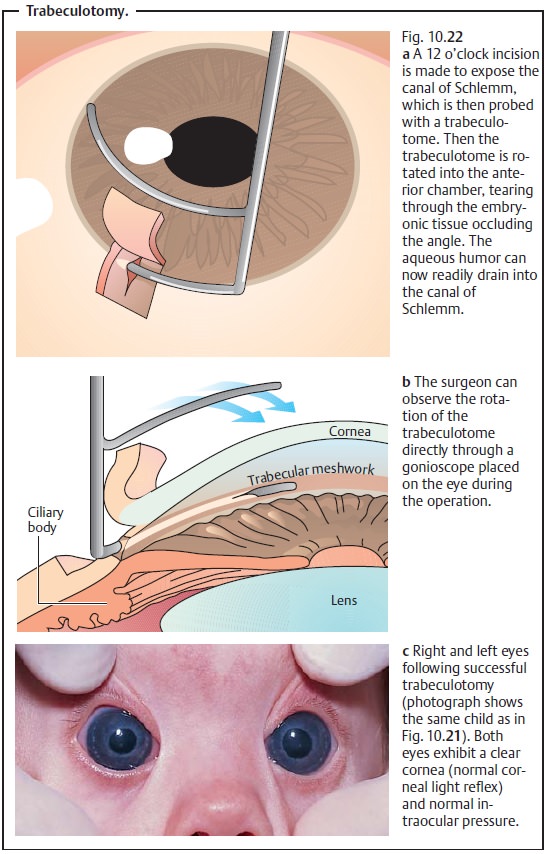
Principle and procedure of trabeculotomy.After a conjunctival flap andsplit-thickness
scleral flap have been raised, access to the canal of Schlemm is gained through
a radial incision, and the canal is probed with a trabeculo-tome. Then the
trabeculotome is rotated into the anterior chamber (Fig. 10.22). This tears through the inner wall
of the canal, the trabecular meshwork, and any embryonic tissue covering it to
open a drainage route for the aqueous humor.
A higher rate of success is attributed to
trabeculotomy when performed as an initial procedure. This operation can also
be performed when the cornea is largely opacified.
Prognosis:
Goniotomies and trabeculotomies are not always successful.Even after apparently successful initial trabecular surgery, these children require a lifetime of follow-up examinations (initially several times a year and later once every year) as elevated intraocular pressure can recur, in which case repeat goniotomy or trabeculotomy is indicated.
Related Topics