Chapter: Ophthalmology: Glaucoma
Glaucoma: Basic Knowledge
Glaucoma
Basic Knowledge
Definition
Glaucoma is a disorder in which increased
intraocular pressure damages the optic nerve. This eventually leads to
blindness in the affected eye.
❖ Primary glaucoma refers to glaucoma that is not caused by other
oculardisorders.
❖ Secondary glaucoma may occur as the result of another ocular disorder oran
undesired side effect of medication or other therapy.
Epidemiology:
Glaucoma is thesecond most
frequent cause of blindnessindeveloping countries after diabetes mellitus.
Fifteen to twenty per cent of all blind persons lost their eyesight as a result
of glaucoma. In Germany, approxi-mately 10% of the population over 40 has
increased intraocular pressure. Approximately 10% of patients seen by
ophthalmologists suffer from glau-coma. Of the German population, 8 million
persons are at risk of developing glaucoma, 800 000 have already developed the
disease (i.e., they have glau-coma that has been diagnosed by an
ophthalmologist), and 80 000 face the risk of going blind if the glaucoma is
not diagnosed and treated in time.
Early detection of glaucoma is one of the
highest priorities for the pub-lic health system.
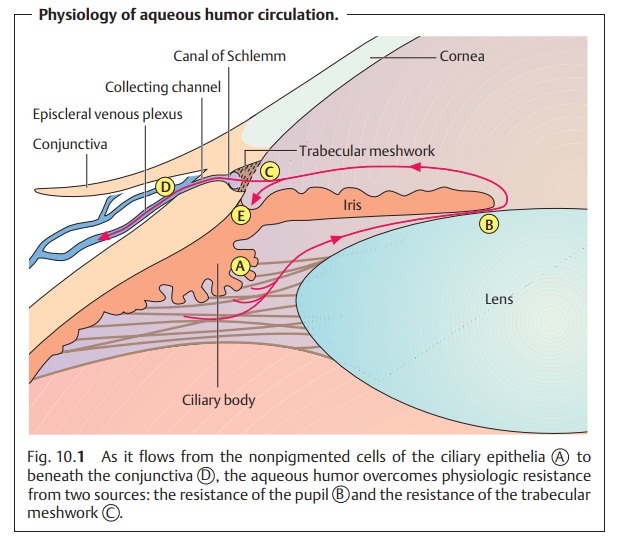
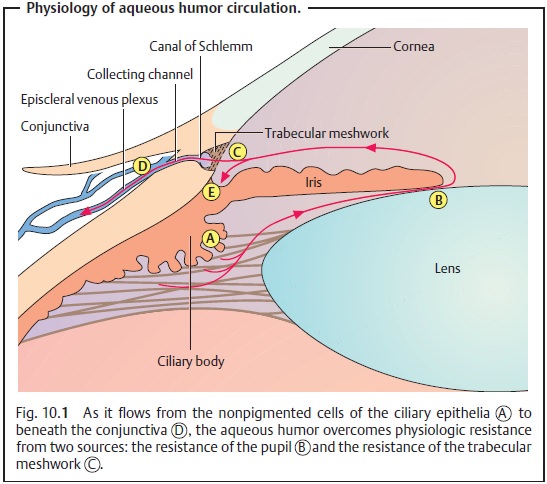
Physiology and pathophysiology of aqueous humor circulation (Fig. 10.1):
The
average normal intraocular pressure of 15
mm Hg in adults is significantly higher than the average tissue pressure in
almost every other organ in the body. Such a high pressure is important for the
optical imaging and helps to ensure several things:
❖Uniformly smooth curvature of the surface of
the cornea.
❖ Constant distance between the cornea, lens,
and retina.
❖ Uniform alignment of the photoreceptors of
the retina and the pigmented epithelium on Bruch’s membrane, which is normally
taut and smooth.
The aqueous humor is formed by the ciliary processes and secreted into the posterior chamber of the eye (Fig. 10.1 [A]). At a rate of about 2 – 6 µl per minute and a total anterior and posterior chamber volume of about 0.2 – 0.4 ml, about 1 – 2% of the aqueous humor is replaced each minute.
The aqueous humor passes through the pupil
into the anterior chamber. As the iris lies flat along the anterior surface of
the lens, the aqueous humor can-not overcome this pupillary resistance (first physiologic resistance; Fig. 10.1 [B]) until sufficient pressure has built up to lift the iris
off the surface of the lens. Therefore, the flow of the aqueous humor from the
posterior chamber into the anterior chamber is not continuous but pulsatile.
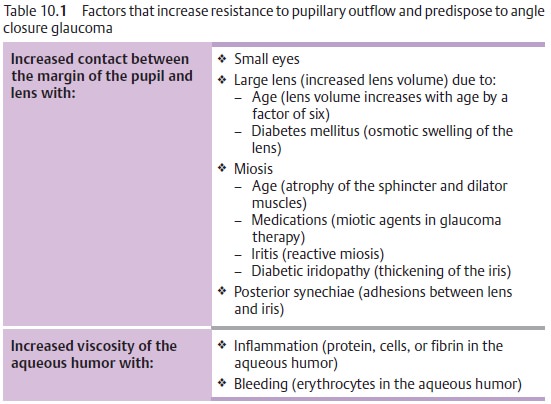
Any increase
in the resistance to pupillary outflow (pupillary
block) leads to an increase in the pressure in the posterior chamber; the
iris inflates anteri-orly on its root like a sail and presses against the
trabecular meshwork (Table 10.2). This is the pathogenesis
of angle closure glaucoma.
Various factors can increase the resistance to
pupillary outflow (Table10.1). The aqueous humor flows out of the angle of the anterior
chamber through two channels:
❖ The trabecular meshwork (Fig. 10.1 [C]) receives about 85% of the out-flow, which then drains into the canal of Schlemm. From here it is conducted by 20 – 30 radial collecting channels into the episcleral venous plexus (D).
❖A uveoscleral vascular system receives about
15% of the outflow, which joins the venous blood (E).
The trabecular meshwork (C) is the second source of physiologic resistance. The trabecular meshwork is a body of loose
sponge-like avascular tissue between the scleral spur and Schwalbe’s line.
Increased resistance in present in open
angle glaucoma.
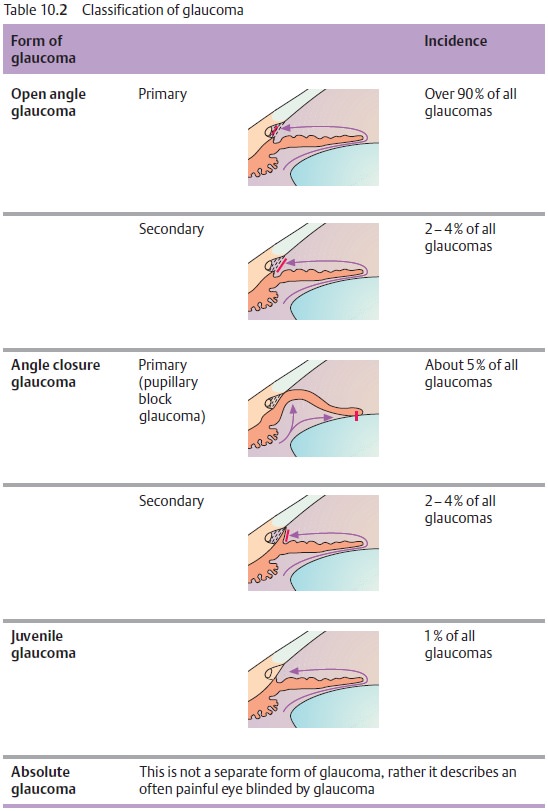
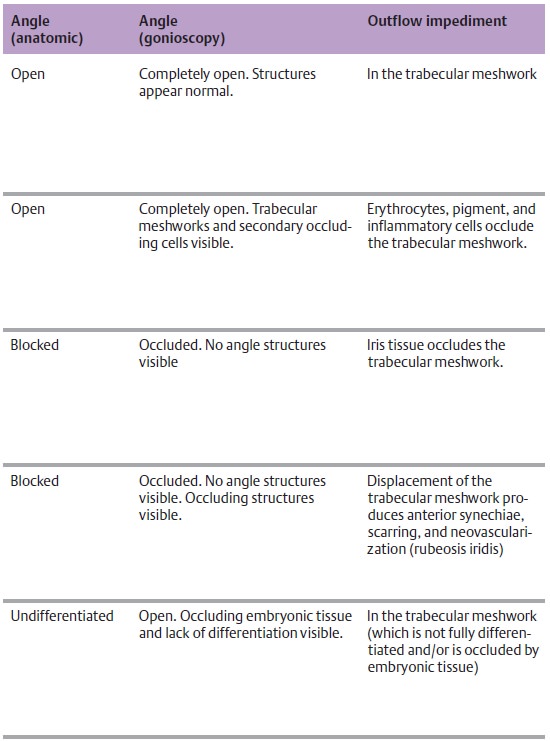
Classification:
Glaucoma can be classified according to the
specificpathophysiology (Table 10.2).
The many various types of glaucoma are nearly all attributable
to increased resistance to outflow and not to heightened secretion of aqueous
humor.
Related Topics