Chapter: Ophthalmology: Glaucoma
Secondary Glaucomas
Secondary Glaucomas
Definition
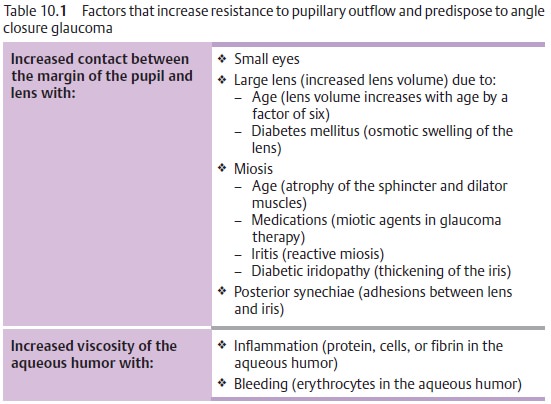
These glaucomas are caused by other ocular diseases of factors
such as inflam-mation, trauma, bleeding, tumors, medication, and physical or
chemical influences (see Table 10.1).
Secondary Open Angle Glaucoma
Definition
The anatomic relationships between the root of
the iris, the trabecular mesh-work, and peripheral cornea are not disturbed.
However, the trabecular mesh-work is congested and the resistance to drainage
is increased.
The most important forms:
Pseudoexfoliative
glaucoma.This form
occursparticularly frequently in Scandinavian countries. Deposits of amorphous
acellular material form throughout the anterior chamber and congest the
trabecular meshwork.
Pigmentary glaucoma.Young myopic men typically are affected. The dis-order is
characterized by release of pigment granules from the pigmentary epithelium of
the iris that congest the trabecular meshwork.
Cortisone glaucoma.Thirty-five to forty per cent of the population react
tothree-week topical or systemic steroid therapy with elevated intraocular
pressure. Increased deposits of mucopolysaccharides in the trabecular mesh-work
presumably increase resistance to outflow; this is reversible when the steroids
are discontinued.
Inflammatory glaucoma.Two mechanismscontribute to the increase inintraocular
pressure:
1.
The viscosity of the
aqueous humor increases as a result of the influx of pro-tein from inflamed
iris vessels.
2.
The trabecular meshwork
becomes congested with inflammatory cells and cellular debris.
Phacolytic glaucoma.This is acute glaucoma in eyes with mature or hyper-mature cataracts.
Denatured lens protein passes through the intact lens cap-sule into the
anterior chamber and is phagocytized. The trabecular meshwork becomes congested
with protein-binding macrophages and the protein itself.
Secondary Angle Closure Glaucoma
Definition
In secondary angle closure glaucoma as in
primary angle closure glaucoma, the increase in intraocular pressure is due to
blockage of the trabecular mesh-work. However, the primary configuration of the
anterior chamber is not the decisive factor.
The most important causes:
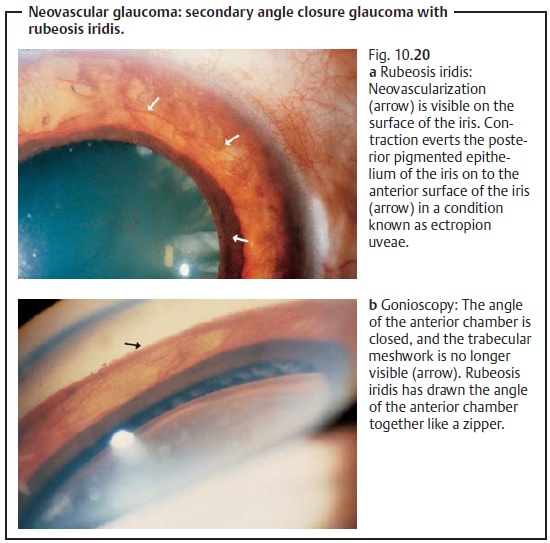
Rubeosis iridis.Neovascularization draws theangle of the anterior chamber
together like a zipper (neovascular glaucoma).
Ischemic retinal disorders such as diabetic retinopathy and retinal vein occlu-sion can lead to
rubeosis iridis with progressive closure of the angle of theanterior chamber.
Other forms of retinopathy or intraocular tumors can also cause rubeosis
iridis. The prognosis for eyes with neovascular glaucoma is poor (see Fig. 10.20a and b).
Trauma.Post-traumatic presence of blood or exudate in
the angle of the ante-rior chamber and prolonged contact between the iris and
trabecular mesh-work in a collapsed anterior chamber (following injury,
surgery, or insuffi-cient treatment of primary angle closure) can lead to anterior
synechiae and angle closure without rubeosis iridis.
Medical therapy of secondary glaucomas is
usually identical to the treatment of primary chronic open angle glaucoma.
Secondary glaucomas may be caused by many
different factors, and the angle may be open or closed. Therefore, treatment
will depend on the etiology of the glaucoma. The underlying disorder is best
treated first. Glaucomas with uveitis (such as iritis or iridocyclitis)
initially are treated conservatively with anti-inflammatory and antiglaucoma
agents. Surgery is indicated where con-servative treatment is not sufficient.
The prognosis for secondary glaucomas is
generally worse than for primary glaucomas.
Related Topics