Chapter: Medical Surgical Nursing: Assessment and Management of Patients With Breast Disorders
Benign Conditions of the Breast
Benign Conditions of the Breast
Benign
breast lesions include fibrocystic changes, fibroadenomas, and cysts.
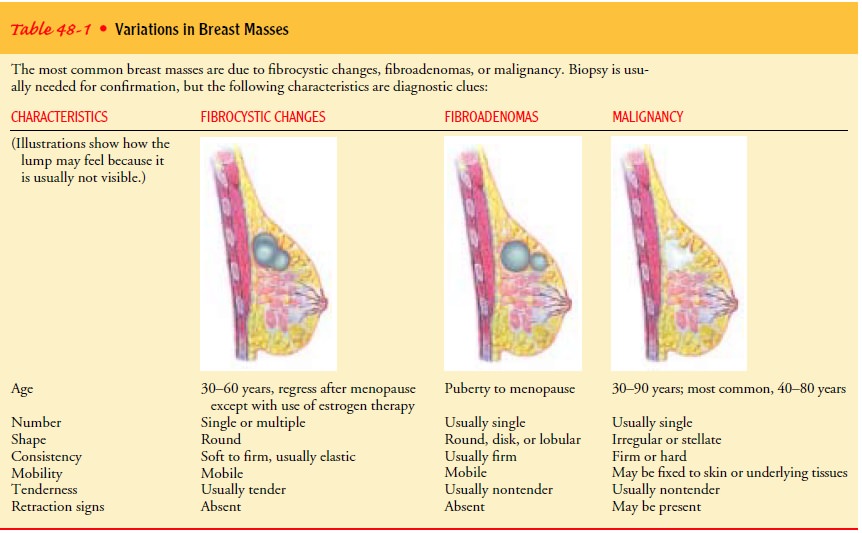
FIBROCYSTIC BREAST CHANGES
Fibrocystic breast changes occur as ducts dilate
and cysts form.This condition occurs most commonly in women ages 30 to 50
years. Although the cause is unknown, estrogen appears to be a factor because
cysts usually disappear after menopause. Cystic areas often fluctuate in size,
depending on the menstrual cycle. They are usually larger premenstrually and
smaller postmenstru-ally because of the retention of fluid in the days
preceding the menstrual period. The cysts may be painless or may become very
tender premenstrually. Occasionally, a patient may report breast pain, which is
usually intermittent and can be shooting or a dull ache (Table 48-1 describes
various breast masses). Breast pain (mastalgia)
is usually related to hormonal fluctuations and their effect on the breasts or
is stimulated by irritation of a nerve in the chest wall from an activity such
as weight training.
Medical Management
If
pain and tenderness are severe, danazol (Danocrine) may be pre-scribed; this
agent has an antiestrogenic effect, therefore decreas-ing breast pain and
nodularity. Danazol is used only in severe cases because of its potential side
effects, which include flushing, vaginitis, and androgenic changes
(virilization).
Nursing Management
The nurse may recommend that the patient wear a supportive bra both day and night for a week except during bathing, decrease her salt and caffeine intake, and take ibuprofen (Motrin, Advil) as needed for its anti-inflammatory actions. Vitamin E supplements or oil of evening primrose (an over-the-counter herbal prepara-tion) may also be helpful, but this recommendation is based on anecdotal information from patients, not on research.
If
diuretic agents or oral contraceptives are prescribed, the pa-tient should know
that symptoms usually recur after these med-ications are discontinued. Patients
should also be reassured that breast pain is rarely indicative of cancer in its
early stages. If the pain is not relieved after menses begins, however, the
woman should see her primary health care provider.
FIBROADENOMAS
Fibroadenomas
are firm, round, movable, benign tumors of the breast that usually affect women
in their late teens to late 30s. These masses are nontender and are sometimes
removed for diag-nostic certainty.
OTHER BENIGN CONDITIONS
Cystosarcoma phyllodes is a fibroepithelial lesion that tends to
growrapidly. It is rarely malignant and is surgically excised. If it is
malignant, mastectomy may follow. Fat
necrosis is a rare condition of the breast that is often related to trauma
from a blow; however, it may be indistinguishable from carcinoma, and the
entire mass is usually excised.
Gigantomastia or macromastia (overly large breasts)
is a prob-lem for some women. Weight loss and various medications have been
tried to little avail. Reduction mammoplasty is an elective procedure for the
patient who is physically or emotionally distressed by this condition. Superficialthrombophlebitis of the
breast (Mondor’s disease) is an uncommoncondition that is usually associated
with pregnancy, trauma, or breast surgery. Pain and redness occur as a result
of a superficial thrombophlebitis in the vein that drains the outer part of the
breast. The mass is usually linear, tender, and erythematous. Treatment
consists of analgesics and heat.
BENIGN PROLIFERATIVE BREAST DISEASE
The
two most common diagnoses of benign
proliferative breastdisease found on biopsy are atypical hyperplasia and
lobular car-cinoma in situ. Both of these diagnoses increase a woman’s risk for
the development of breast cancer. Atypical
hyperplasia is an abnormal increase in the ductal or lobular cells in the
breast and is usually found incidentally in mammographic abnormalities.
Atypical hyperplasia increases a woman’s risk for breast cancer about 10% to
20% over a period of 10 years; the risk is greater for premenopausal women and
decreases significantly after meno-pause (Hulka & Moorman, 2001). Lobular carcinoma in situ (LCIS) is
usually an incidental finding in breast tissue because it cannot be seen on
mammography and does not form a palpable lump. Historically, LCIS was
considered a premalignant condi-tion, and treatment consisted of a bilateral
prophylactic mastec-tomy; however, current research indicates that LCIS is a
marker for the risk for invasive breast cancer, which can either be ductal or
lobular in origin and can develop in either breast. LCIS in-creases a woman’s
risk for breast cancer by about 25% to 40% over a period of 25 years, and the
risk does not diminish with time (Frykberg, 1999).
For
women at higher risk, a newer technique called ductal lavage may be used. It
involves inserting a microcatheter through the nipple while instilling saline
and retrieving the fluid for analy-sis. It has been shown to identify atypical
cells in this population (Dooley, Ljung, Veronisi et al., 2001), providing
women with more information regarding their risk. This procedure, which is done
in the office and is well tolerated, was found to be more use-ful at detecting
cellular changes within the breast tissue. Contin-ued research is needed to
determine its benefit in screening and early detection for women at high risk.
Medical Management
After
a woman has been diagnosed with a benign proliferative condition such as
atypical hyperplasia or LCIS, she has three treatment options: long-term
surveillance (observation), bilat-eral prophylactic mastectomy (a risk-reducing
surgical proce-dure), or chemoprevention (using a medication to decrease the
risk of developing breast cancer). Each of these options may be offered by a
breast specialist, usually associated with a compre-hensive breast center. Most
women choose surveillance and at-tempt to modify certain risk factors, such as
diet, exercise, and alcohol consumption. For some women, however, prophylactic
mastectomy may be an option; taking tamoxifen (Nolvadex) may be an option for
others. Tamoxifen has recently been shown to decrease the incidence of invasive
breast cancer for high-risk women by 49% (Fisher, Constantino, Wickerham et
al., 1998). The risks and benefits of each of these options must be explained
so that the woman can make a careful decision.
Related Topics