Chapter: Psychiatric Mental Health Nursing : Child and Adolescent Disorders
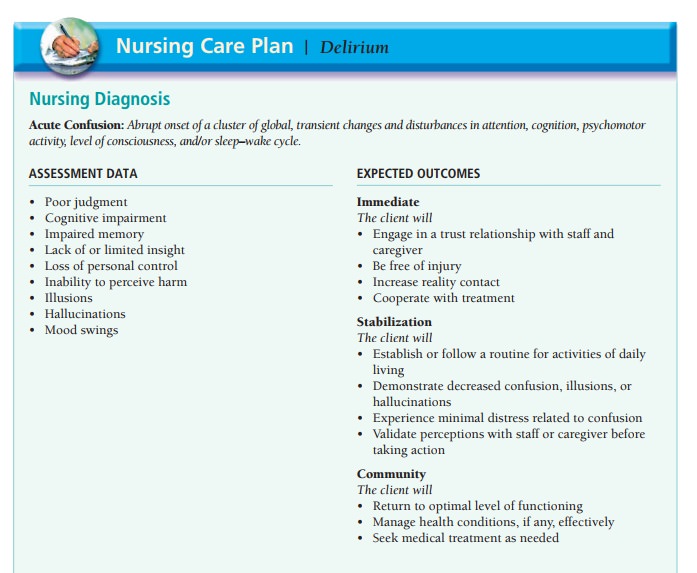
Application of the Nursing Process: Delirium
APPLICATION OF THE NURSING
PROCESS: DELIRIUM
Nursing care for clients with delirium focuses on meeting their physiologic and psychologic needs and maintaining their safety. Behavior, mood, and level of consciousness of these clients can fluctuate rapidly throughout the day. Therefore, the nurse must assess them continuously to recognize changes and to plan nursing care accordingly.
Assessment
History
Because the causes of delirium are often related to medical
illness, alcohol, or other drugs, the nurse obtains a thor-ough history of
these areas. The nurse may need to obtain information from family members if a
client’s ability to provide accurate data is impaired.
Information about drugs should include prescribed medications,
alcohol, illicit drugs, and over-the-counter med-ications. Although many people
perceive prescribed and over-the-counter medications as relatively safe,
combinations or standard doses of medications can produce delirium, espe-cially
in older adults.
General Appearance and Motor Behavior
Clients with delirium often have a disturbance of psychomo-tor
behavior. They may be restless and hyperactive, frequently picking at
bedclothes or making sudden, uncoordinated attempts to get out of bed.
Conversely, clients may have slowed motor behavior, appearing sluggish and
lethargic with little movement.
Speech also may be affected, becoming less coherent and more
difficult to understand as delirium worsens. Clients may perseverate on a
single topic or detail, may be rambling and difficult to follow, or may have
pressured speech that is rapid, forced, and usually louder than normal. At
times, cli-ents may call out or scream, especially at night.
Mood and Affect
Clients with delirium often have rapid and unpredictable mood
shifts. A wide range of emotional responses is possi-ble, such as anxiety,
fear, irritability, anger, euphoria, and apathy. These mood shifts and emotions
usually have noth-ing to do with the client’s environment. When clients are
particularly fearful and feel threatened, they may become combative to defend
themselves from perceived harm.
Thought Process and Content
Although clients with delirium have changes in cognition, it is
difficult for the nurse to assess these changes accurately and thoroughly.
Marked inability to sustain attention makes it difficult to assess thought
process and content. Thought content in delirium often is unrelated to the
situation, or speech is illogical and difficult to understand. The nurse may
ask how clients are feeling, and they will mumble about the weather. Thought
processes often are disorganized and make no sense. Thoughts also may be
fragmented (disjointed and incom-plete). Clients may exhibit delusions,
believing that their altered sensory perceptions are real.
Sensorium and Intellectual Processes
The primary and often initial sign of delirium is an altered level
of consciousness that is seldom stable and usually fluctuates throughout the
day. Clients usually are oriented to person but frequently disoriented to time
and place. They demonstrate decreased awareness of the environ-ment or
situation and instead may focus on irrelevant stimuli such as the color of the
bedspread or the room. Noises, people, or sensory misperceptions easily
distract them.
Clients cannot focus, sustain, or shift attention effec-tively, and
there is impaired recent and immediate memory (APA, 2000). This means the nurse
may have to ask ques-tions or provide directions repeatedly. Even then, clients
may be unable to do what is requested.
Clients frequently experience misinterpretations, illu-sions, and
hallucinations. Both misperceptions and illu-sions are based on some actual stimuli
in the environment: clients may hear a door slam and interpret it as a gunshot
or see the nurse reach for an intravenous bag and believe the nurse is about to
strike them. Examples of common illusions include clients believing that
intravenous tubing or an electrical cord is a snake and mistaking the nurse for
a family member. Hallucinations are most often visual: cli-ents “see” things
for which there is no stimulus in reality. Some clients, when more lucid, are
aware that they are experiencing sensory misperceptions. Others, however,
actually believe their misinterpretations are correct and cannot be convinced
otherwise.
Judgment and Insight
Judgment is impaired. Clients often cannot perceive poten-tially
harmful situations or act in their own best interests. For example, they may
try repeatedly to pull out intrave-nous tubing or urinary catheters; this
causes pain and interferes with necessary treatment.
Insight depends on the severity of the delirium. Cli-ents with mild
delirium may recognize that they are con-fused, are receiving treatment, and
will likely improve. Those with severe delirium may have no insight into the
situation.
Roles and Relationships
Clients are unlikely to fulfill their roles during the course of
delirium. Most regain their previous level of function-ing, however, and have
no longstanding problems with roles or relationships.
Self-Concept
Although delirium has no direct effect on self-concept, cli-ents
often are frightened or feel threatened. Those with some awareness of the
situation may feel helpless or pow-erless to do anything to change it. If
delirium has resulted from alcohol, illicit drug use, or overuse of prescribed
medications, clients may feel guilt, shame, and humilia-tion or think, “I’m a
bad person; I did this to myself.” This would indicate possible long-term
problems with self-concept.
Physiologic and Self-Care Considerations
Clients with delirium most often experience disturbed sleep–wake
cycles that may include difficulty falling asleep, daytime sleepiness,
nighttime agitation, or even a com-plete reversal of the usual daytime
waking/nighttime sleep-ing pattern (APA, 2000). At times, clients also ignore
or fail to perceive internal body cues such as hunger, thirst, or the urge to
urinate or defecate.
Data Analysis
The primary nursing diagnoses for clients with delirium are as
follows:
·
Risk for Injury
·
Acute Confusion
Additional diagnoses that are commonly selected based on client
assessment include the following:
·
Disturbed Sensory Perception
·
Disturbed Thought Processes
·
Disturbed Sleep Pattern
·
Risk for Deficient Fluid Volume
Risk for Imbalanced Nutrition: Less Than Body Requirements
Outcome Identification
Treatment outcomes for the client with delirium may include the
following:
·
The client will be free of injury.
·
The client will demonstrate increased orientation and reality
contact.
·
The client will maintain an adequate balance of activity and rest.
·
The client will maintain adequate nutrition and fluid balance.
·
The client will return to his or her optimal level of functioning.
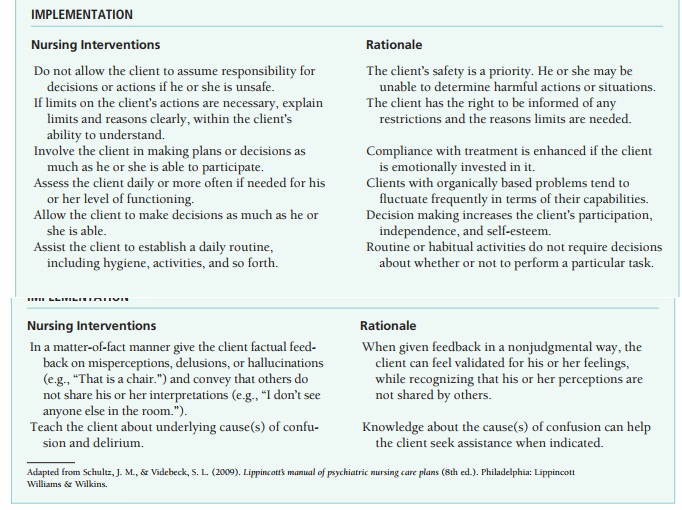
Intervention
Promoting the Client’s Safety
Maintaining the client’s safety is the priority focus of nurs-ing
interventions. Medications should be used judiciously because sedatives may
worsen confusion and increase the risk for falls or other injuries (Samuels
& Neugroschl, 2005).
The nurse teaches clients to request assistance for activ-ities
such as getting out of bed or going to the bathroom. If clients cannot request
assistance, they require close super-vision to prevent them from attempting
activities they can-not perform safely alone. The nurse responds promptly to
calls from clients for assistance and checks clients at fre-quent intervals.
If a client is agitated or pulling at intravenous lines or
catheters, physical restraints may be necessary. Use of restraints, however,
may increase the client’s fears or feelings of being threatened, so restraints
are a last resort. The nurse first tries other strategies such as having a
fam-ily member stay with the client to reassure him or her.
Managing the Client’s Confusion
The nurse approaches these clients calmly and speaks in a clear low
voice. It is important to give realistic reassurance to clients, such as
“I know things
are upsetting and confusing right now, but your confusion should clear as you
get better.” (validating/giving information)
The nurse provides orienting cues when talking with cli-ents, such
as calling them by name and referring to the time of day or expected activity.
For example, the nurse might say,
“Good morning, Mrs. Jones. I see you are awake and look ready for breakfast.” (giving information)
Reminding the client of the nurse’s name and role repeat-edly may
be necessary, such as
“My name is
Sheila, and I’m your nurse today. I’m here now to walk in the hall with you.” (re-ality
orientation)
Orienting objects such as a calendar and clock in the client’s room
are useful.
Often, the use of touch reassures clients and provides contact with
reality. It is important to evaluate each client’s response to touch rather
than to assume all clients wel-come it. A client who smiles or draws closer to
the nurse when touched is responding positively. The fearful client may
perceive touch as threatening rather than comforting and startle or draw away.
Clients with delirium can experience sensory overload, which means
more stimulation is coming into the brain than they can handle. Reducing
environmental stimulation is helpful because these clients are distracted and
overstim-ulated easily. Minimizing environmental noises, including television
or radio, should calm them. It is also important to monitor response to
visitors. Too many visitors or more than one person talking at once may
increase the client’s confusion. The nurse can explain to visitors that the
client will best tolerate quiet talking with one person at a time.
The client’s room should be well lit to minimize environ-mental
misperceptions. When clients experience illusions or misperceptions, the nurse
corrects them matter-of-factly. It is important to validate the client’s
feelings of anxiety or fear generated by the misperception but not to reinforce
that misperception. For example, a client hears a loud noise in the hall and
asks the nurse, “Was that an explosion?”
The nurse might respond,
“No, that was a
cart banging in the hall. It was really loud, wasn’t it? It startled me a
little when I heard it.” (presenting reality/validat-ing feelings)
Promoting Sleep and Proper Nutrition
The nurse monitors the client’s sleep and elimination pat-terns and
food and fluid intake. Clients may require prompt-ing or assistance to eat and
drink adequate food and fluids. It may be helpful to sit with clients at meals
or to frequently offer fluids. Family members also may be able to help cli-ents
to improve their intake. Assisting clients to the bath-room periodically may be
necessary to promote elimination if clients do not make these requests
independently.
Promoting a balance of rest and sleep is important if clients are
experiencing a disturbed sleep pattern. Dis-couraging or limiting daytime
napping may improve abil-ity to sleep at night. It is also important for
clients to have some exercise during the day to promote nighttime sleep.
Activities could include sitting in a chair, walking in the hall, or engaging
in diversional activities (as possible).
Evaluation
Usually, successful treatment of the underlying causes of delirium
returns clients to their previous levels of func-tioning. Clients and
caregivers or family must understand what health care practices are necessary
to avoid a recur-rence. This may involve monitoring a chronic health
con-dition, using medications carefully, or abstaining from alcohol or other
drugs.
Related Topics