Chapter: Clinical Anesthesiology: Perioperative & Critical Care Medicine: Anesthetic Complications
Anesthetic Complications: Mortality and Brain Injury
MORTALITY AND BRAIN INJURY
Trends in anesthesia-related death and brain dam-age have been tracked
for many years. In a Closed Claims Project report examining claims in the
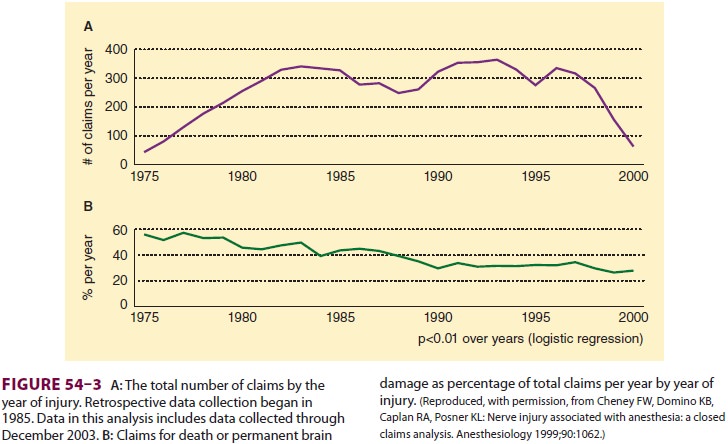
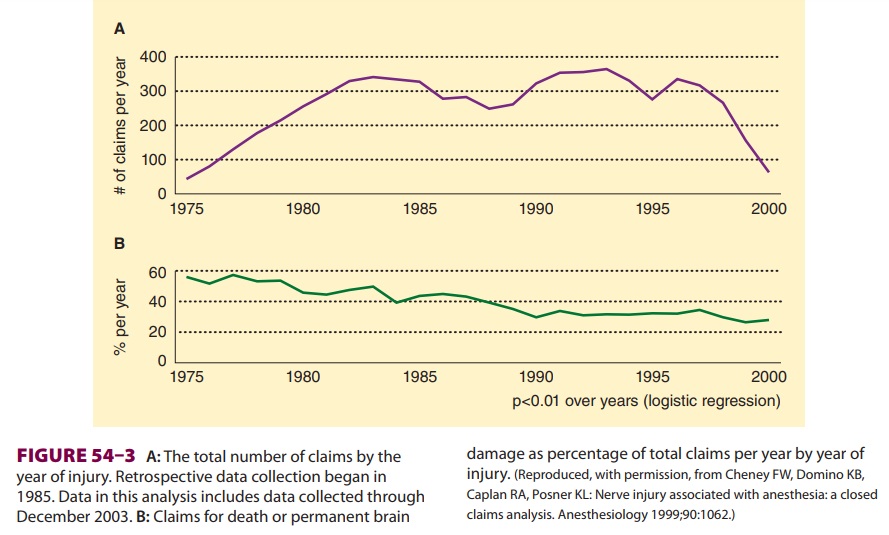
period between 1975 and 2000, there were 6750
claims (Figure 54–3A and B), 2613 of which were for brain injury or death. The
proportion of claims for brain injury or death was 56% in 1975, but had
decreased to 27% by 2000. The primary pathological mechanisms by which these
outcomes occurred were related to cardiovascular or respiratory prob-lems.
Early in the study period, respiratory-related damaging events were responsible
for more than 50% of brain injury/death claims, whereas cardio-vascular-related
damaging events were responsible for 27% of such claims; however, by the late
1980s, the percentage of damaging events related to respi-ratory issues had
decreased, with both respiratory and cardiovascular events being equally likely
to contribute to severe brain injury or death. Respira-tory damaging events
included difficult airway, esophageal intubation, and unexpected extubation.
Cardiovascular damaging events were usually multi-factorial. Closed claims
reviewers found that anes-thesia care was substandard in 64% of claims in which
respiratory complications contributed to brain injury or death, but in only 28%
of cases in which the primary mechanism of patient injury was cardiovascular in
nature. Esophageal intubation, premature extubation, and inadequate ventilation
were the primary mechanisms by which less than optimal anesthetic care was
thought to have contrib-uted to patient injury related to respiratory events.The relative decrease in causes of death being attributed to respiratory
rather cardiovasculardamaging events during
the review period was attributed to the increased use of pulse oximetry and
capnometry. Consequently, if expired gas analysis was judged to be adequate,
and a patient suffered brain injury or death, a cardiovascular event was more
likely to be considered causative.
A 2010 study examining the NHS Litiga-tion Authority dataset noted that airway-related claims led to higher awards and poorer outcomes than did nonairway-related claims. Indeed, airway manipulation and central venous catheter ization claims in this database were most associated with patient death. Trauma to the airway also generates significant claims if esophageal or tracheal rupture occur. Postintubation mediastinitis should always be considered whenever there are repeated unsuc-cessful airway manipulations, as early intervention presents the best opportunity to mitigate any inju-ries incurred.
Related Topics