Chapter: Medicine and surgery: Endocrine system
AddisonŌĆÖs disease - Adrenal axis
AddisonŌĆÖs disease
Definition
First described by Thomas Addison in 1857, AddisonŌĆÖs disease is primary adrenal insufficiency.
Aetiology
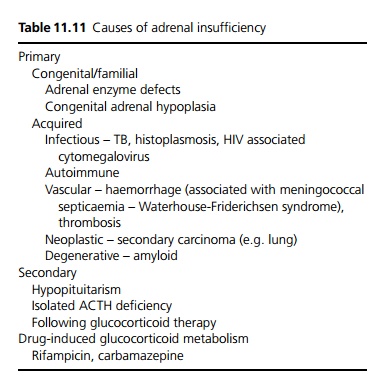
In Western countries autoimmune disease is the commonest cause (80%). It is familial, and associated with other organ specific autoimmune diseases, especially thyroid failure (Schmidt syndrome), autoimmune gastritis, pernicious anaemia and vitiligo. Presence of HLA-B8 association carries a x12 risk of developing disease. Worldwide, tuberculosis is still a very important cause (see Table 11.11).
Pathophysiology
The mineralocorticoids (90% activity by aldosterone,
some by cortisol) act on the kidneys to conserve sodium by increasing Na+ / K+ exchange in the distal tubules and collecting ducts. In AddisonŌĆÖs disease, gradual loss of these hormones causes increased sodium and water loss with a consequent decrease in extracellular fluid volume. Failure to exchange Na+ for H+ ions can lead to a mild acidosis.
The glucocorticoids (cortisol) allow gluconeogenesis to maintain glucose concentrations between meals, and mediate protein and fat mobilisation from the tissues. Reduced cortisol may lead to symptomatic hy-poglycaemia.
Lack of cortisol feedback leads to increased ACTH (adrenocorticotrophin) secretion from the anterior pituitary. When ACTH is secreted by the anterior pituitary, other hormones are also secreted such as ╬▓-endorphin and melanocyte-stimulating hormone (MSH) causing skin pigmentation.
Once mineralocorticoid secretion ceases completely, the patient will die within 2 weeks if not treated, from progressive weakness and eventual shock.
Clinical features
Patients present with gradual onset of weakness, tiredness and fatigue. There are often gastrointestinal complaints such as anorexia, nausea, vomiting, abdominal pain, constipation or diarrhoea. The patient may report salt craving.
Examination reveals weight loss, hyperpigmentation especially in mouth, skin creases and pressure areas. Chronic dehydration leads to general and especially postural hypotension.
Complications
Renal failure due to decreased perfusion. Sudden cardiac arrest or arrhythmias due to electrolyte imbalance.
Investigations
Hyponatremia, hyperkalemia and a hyperchloraemic acidosis due to mineralocorticoid deficiency. Glucose should be measured to detect hypoglycaemia.
Screening can be performed by measurement of early morning cortisol and 24 hour urinary cortisol.
Primary adrenal insufficiency is confirmed by use of the short Synacthen (ACTH analogue) test. Cortisol levels are measured before and 30 mins after admin-istration of synacthen and show a low base line and a lack of rise in AddisonŌĆÖs Disease. Adrenal insufficiency that results from ACTH deficiency (secondary and tertiary adrenal insufficiency) will result in an appropriate rise in cortisol following Synacthen. A long Synacthen test using a depot injection and repeated cortisol samples over a 24-hour period is used to distinguish between AddisonŌĆÖs disease (primary adrenal failure) and adrenal suppression.
Management
Chronic adrenal insufficiency is treated with glucocorticoids and mineralocorticoids. Patients require significant education about the illness and how to manage coexisting illness or stress, such as at the time of operations when increased steroids may be required. Parenteral steroids are needed if vomiting occurs. All patients requiring replacement steroids should carry a steroid (blue) card.
Related Topics