Chapter: Medicine and surgery: Endocrine system
Pituitary adenomas
Pituitary adenomas
Definition
Pituitary adenomas are benign slow growing tumours arising from the anterior pituitary.
Aetiology
The cause of most pituitary adenomas is unknown. Gene mutations have been characterised in some pituitary ade-nomas, for example in the condition multiple endocrine neoplasia (MEN) type 1 tumours including pituitary adenomas occur due to the loss of tumour suppressor genes.
Pathophysiology
Seventy per cent of pituitary adenomas are functioning, i.e. hormone secreting. These tend to present earlier than the other 30% non-functioning tumours.
Clinical features
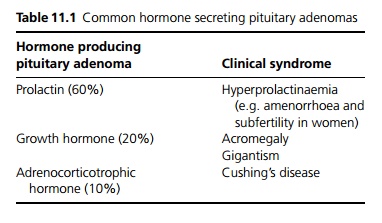
Pituitary adenomas produce symptoms through local pressure such as headache, and visual loss due to pressure on the optic chiasm (bilateral temporal heminanopia). Continuing growth disrupts other hormone secretion and can result in hypopituitarism. Symptoms may also result from the effects of hormone excess (see Table 11.1).
Macroscopy
Tumours less than 1 cm in diameter without enlargement of, or extension outside the pituitary fossa are defined as microadenomas.
Tumours larger than 1 cm in diameter are called macroadenomas and may cause pituitary fossa enlargement.
Tumours Ôëą1ÔÇô2 cm may extend outside the fossa towards the hypothalamus and optic chiasm, laterally into the cavernous sinus or downwards into the sphenoid sinus.
Investigations
A mass within the sella turcica (pituitary fossa) may be identified on plain skull X-ray.
MRI scanning using gadolinium contrast is the imaging modality of choice. Microadenomas take up less contrast and macroadenomas take up more contrast.
If a pituitary mass is identified, hormone assays should be undertaken to identify functioning adenomas. Testing also helps identify any associated hypopituitarism, with stimulation or suppression testing where appropriate.
Management
For prolactinomas medical treatment with a dopaminergic drug is the treatment of choice (see section on Hyperprolactinaemia).
For other pituitary adenomas, transsphenoidal resection is the treatment of choice, with postoperative radiotherapy for patients where complete resection has not been possible. Major postoperative complications include CSF leakage, meningitis or visual impairment, which are most frequent in patients undergoing large resections. Transient diabetes insipidus or syndrome of inappropriate anti-diuretic hormone (SIADH) may also occur. Increasingly asymptomatic pituitary adenomas are found at incidental imaging. In elderly or infirm patients surgery may not be appropriate.
All patients require regular assessment for hormone deficiencies with replacement therapy used as necessary.
Related Topics