Chapter: Paediatrics: Neonatology
Paediatrics: Neonatal jaundice
Neonatal jaundice
Jaundice is common (60% term, 80%
preterm in first week), and is usually unconjugated. Significant jaundice may
indicate un-derlying disease. High serum unconjugated free bilirubin is
neurotoxic and can cause kernicterus (deafness, athetoid cerebral palsy (CP),
seizures).
Physiological jaundice
Common and appears after 24hr,
peaks around day 3ŌĆō4, and usually re-solves by 14 days. It is due to immaturity
of hepatic bilirubin conjugation, but poor feeding (particularly in breast-fed
infants) can also contribute. Jaundice progresses in a cephalic-caudal
direction.
Measure bilirubin (transcutaneous
or serum) in babies with jaundice. Action is required when serum bilirubin (SBR)
is above gestation and age cut-offs (e.g. >300┬Ąmol/l in term infant at 72hr)
or rapidly rising.
Causes of elevated SBR
Exaggerated
physiological jaundice (e.g. preterm, bruising);
sepsis; haemolytic disorders; hepatic disease.
Treatment of elevated SBR
┬Ę
Stop
bilirubin rising to level that may cause kernicterus.
┬Ę
Treat
any underlying cause, e.g. sepsis.
┬Ę
Start
ŌĆśblue lightŌĆÖ phototherapy (converts bilirubin to water-soluble form that can
then be excreted in urine).
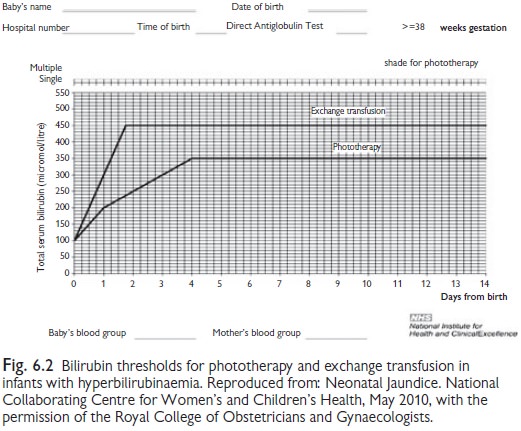
┬Ę
Use
age/gestation specific charts to determine level to start phototherapy (see
Fig. 6.2). Be aware of risk factors (family history, exclusive breast feeding,
Rh or blood group incompatibility).
┬Ę
Measure
SBR frequently (4ŌĆō24-hourly depending on circumstances) and stop when falls
below treatment level.
┬Ę
Ensure
adequate hydration.
┬Ę
Cover
eyes (phototherapy side effects: ŌĆśfallŌĆÖ or ŌĆśriseŌĆÖtemperature; eye damage;
diarrhoea; dehydration; rash; separation from mother).
┬Ę
Exchange
transfusion ┬▒ intravenous immunoglobulin (IVIG) if very high SBR (e.g. >450┬Ąmol/L
in term infant at 48hr) or rapid rise (>8.5┬Ąmol/L/hr).
┬Ę
In the
UK the National Institute of Clinical Excellence (NICE) has produced guidance
on investigation and management of newborn jaundice (see Fig 6.2)ŌĆöthe full
guideline also includes gestation specific treatment thresholds.
Jaundice in the first 24hrs
Assume it is pathological. Start
phototherapy. Check SBR, FBC, direct coombs test (DCT), and blood group.
Consider septic screen/ TORCH.
Causes
Haemolysis (e.g. Rh disease), red cell enzyme defects (e.g. G6PD deficiency), red cell membrane defects (congenital spherocytosis, ellipto-cytosis), sepsis, severe bruising.
Prolonged jaundice (>14 days in term infant; >21 days in preterm)
All infants require investigation
and measurement of conjugated bilirubin. If conjugated hyperbilirubinaemia
present, further specialized investigation will be required. Ask about pale
stools/dark urine.
Causes
Breastfeeding (benign,
self-limiting, and usually resolves by 12wks), enclosed bleeding (e.g. cephalhaematoma), prematurity, haemolysis,
sep-sis, hypothyroidism, conjugated jaundice, hepatic enzyme disorders (e.g.
CriglerŌĆōNajjar Syndrome, LucyŌĆōDriscoll disease).
Initial investigations
SBR
(total and conjugated), U&E, FBC, DCT, blood group, thyroid function test (TFTs), LFTs, and glucose.
Treatment
Depends on cause.
Rarely phototherapy is
beneficial, e.g.
CriglerŌĆōNajjar Syndrome.
Conjugated jaundice (conjugated SBR >25┬Ąmol/L))
Stools may be clay-coloured in
obstructive jaundice.
Causes
Sepsis, TPN, biliary tract
obstruction (e.g. biliary atresia, choledo-chal cyst), viral hepatitis; TORCH
infections, ╬▒1-antitrypsin deficiency, cystic fibrosis, inspissated
bile syndrome after haemolytic disease, galac-tosaemia, other inherited
metabolic disease, idiopathic giant cell hepatitis.
Initial investigations
As for
prolonged jaundice. Further investigations
include radiology, enzyme testing, viral serology, liver biopsy, histology.
Treatment
Depends on cause.
Related Topics