Chapter: Paediatrics: Neonatology
Paediatrics: Necrotizing enterocolitis
Necrotizing enterocolitis
Incidence
The most common neonatal surgical
emergency. Incidence 1ŌĆō3/1000 live births (5ŌĆō10% in VLBW infants). Incidence is
reduced 6-fold in preterm infants fed breast milk. Typically a sporadic
condition affecting preterm infants (790% of cases), but can be epidemic or
occur in term infants. The disease may just involve an isolated area of gut, or
be extensive. Distal ter-minal ileum and proximal colon are most frequently
affected. Multi-organ failure is associated with diffuse disease.
Cause
Multifactorial. Severe intestinal
necrosis is end result of an exaggerated immune response within the immature
bowel leading to inflammation and tissue injury. NEC rarely occurs before milk
feeding commences, but tim-ing of first feed appears not to be relevant.
Predisposing factors:
ŌĆó
Prematurity.
ŌĆó
IUGR
(causes chronic bowel ischaemia).
ŌĆó
Hypoxia.
ŌĆó
Polycythaemia.
ŌĆó
Exchange
transfusion.
ŌĆó
Hyperosmolar
milk feeds.
Presentation
Most common in the second week
after birth.
Early
ŌĆó
Non-specific
illness.
ŌĆó
Vomiting/bilious
aspirate from gastric tube.
ŌĆó
Poor
feed toleration (increasing gastric aspirates).
ŌĆó
Abdominal
distension.
Late
ŌĆó
Additional
abdominal tenderness.
ŌĆó
Blood,
mucus, or tissue in stools.
ŌĆó
Bowel
perforation.
ŌĆó
Shock.
ŌĆó
DIC;
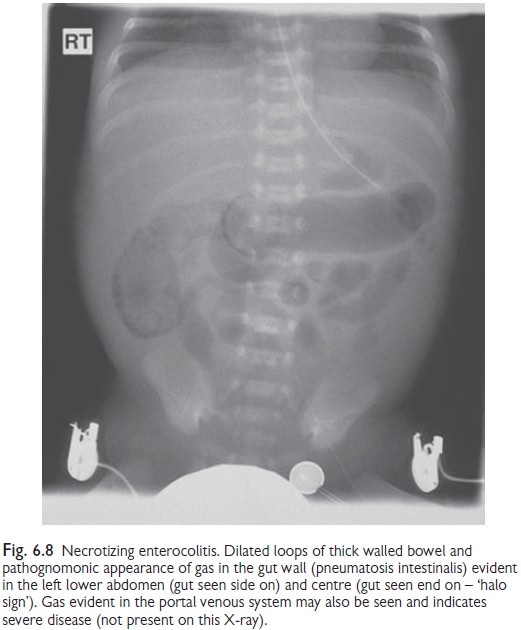
multi-organ failure. AXR shows intestinal distension (see Fig. 6.8).
ŌĆó
Pneumatosis
intestinalis.
ŌĆó
Hepatic
portal venous gas.
ŌĆó
Signs
of intestinal perforation, e.g. free peritoneal gas or gas outlining of falciform
ligament (ŌĆśfootballŌĆÖ sign).
Management
ŌĆó
Prophylaxis: antenatal steroids and breast milk
are protective. Emerging evidence for
prevention by administration of probiotic bacteria.
ŌĆó
Investigations: FBC; U&E; creatinine;
coagulation screen; albumin; blood gas;
blood culture; AXR; Group and cross match.
ŌĆó
Stop
milk feeds for 10ŌĆō14 days. Insert gastric tube on free drainage.
ŌĆó
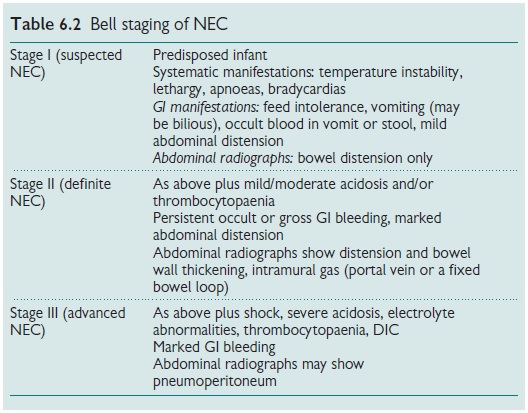
ŌĆśBell
stagingŌĆÖ (see Table 6.2) may be useful in grading severity.
ŌĆó
IV
antibiotics for 10ŌĆō14 days, e.g. benzylpenicillin, gentamicin, and
metronidazole.
ŌĆó
Systemic support: e.g. assisted ventilation, correct
BP and DIC, parenteral nutrition
(PN).
ŌĆó
Surgical opinion: indications for surgery are GI
perforation, deterioration despite
above medical treatment (necrotic bowel likely), GI obstruction secondary to
stricture formation (late). If localized disease, surgical resection of
involved bowel with primary repair.
If more extensive, two stage
repair with bowel resection(s) and enterostomy, followed later by intestinal
re-anastomosis.
Prognosis
Overall mortality is 722%.
Increased mortality is associated with:
ŌĆó
VLBW.
ŌĆó
Extensive
intestine involvement.
ŌĆó
Multi-organ
failure.
ŌĆó
Intrahepatic
portal gas.
Extensive bowel resection may result in short bowel syndrome. Excellent prognosis is seen in those who respond to medical treatment, but subse-quent stricture may develop.
Related Topics