Chapter: Modern Medical Toxicology: Organic Poisons (Toxins): Venomous Bites and Stings
Marine Venomous Creatures
MARINE VENOMOUS CREATURES
The
sea is host to a wide variety of venomous creatures which sting or bite, and
are a special threat to swimmers and divers. Marine envenomations have risen
sharply in incidence over the last few decades owing to an increase in
popularity of recreational diving and other water related sports.
Marine Vertebrates
Approximately
225 species of marine fish are known to be venomous. These include the
stingray, scorpionfish, lion- or zebra-fish, stonefish, weeverfish, toadfish,
stargazer, and certain catfish, sharks, ratfish, and surgeonfish. The most
common marine envenomations are caused by fish belonging to family Scorpaenidae
of class Osteichthyes and order Perciformes. Venomous fish produce envenomation
by means of their spines, fins, or caudal stings.
In
most cases, the stung victim experiences severe burning pain and swelling
within seconds of the sting. Systemic symp-toms include nausea, vomiting,
hypotension, and rarely cardiac arrhythmias. Stings from a stingray can result
in severe lacera-tions with tendency to necrosis. There is intense pain,
associated with paraesthesias, nausea, vomiting, abdominal pain, cardiac
arrhythmias, and convulsions. Limb paralysis may be seen with severe
envenomations.
Treatment
involves the following measures:
·
Soaking the affected limb in hot
water (110° to 115° F).
·
Paracetamol, salicyclates,
non-steroidal anti-inflammatory drugs, or opiate analgesic for pain, depending
on the severity.
·
Tetanus prophylaxis.
·
Wound care.
·
Supportive measures.
Marine Invertebrates
·
There are two important phyla of venomous marine
inverte-brates: Coelenterata and Echinodermata. Less common inver-tebrates
which cause envenomation include molluscs such as cone shells and octopuses.
Coelenterates
account for most of the reported cases of marine envenomations around the
world, and comprise more than 9,000 species of which approximately 100
belonging to Cnidaria are venomous. The Cnidaria are subdivided into 3 classes:
Hydrozoa, Schiphozoa, and Anthozoa:
· Hydrozoa
Portuguese
man-o’-war (Physalia sps).
· Schiphozoa
Jellyfish
(“box jelly”, “fire medusa”) (Chironex
fleckeri)
Sea
nettle.
· Anthozoa
Sea
anemone
Coral.
Most
of the Cnidaria possess stinging structures called nema-tocysts or cnidocytes,
which are poisonous dart-like structures, tightly coiled and enclosed within
venom sacs. Following external contact, they are expelled from the sacs,
injecting venom as they penetrate the flesh of their prey. The venom is a
complex mixture of serotonin, histamine, bradykinin, haemolysin,
pros-taglandins, hyaluronidase, phosphodiesterases, fi brinolysin, RNAase,
DNAase, adenosine triphosphatase, alkaline and acid proteases, as well as
alkaline and acid phosphatases.
Envenomation
usually results in local burning pain with erythematous or violaceous lesions,
and regional lymphad-enopathy. Erythema nodosum, arthralgias, and anaphylactoid
reactions have also been reported. Delayed hypersensitivity reactions may
occur, consisting of a pruritic erythematous maculopapular rash appearing at
the initial tentacle contact points, usually in 7 to 14 days after
envenomation. The reac-tions spontaneously resolve in some patients, while
others recover following treatment with oral antihistamines and topical
corticosteroids.
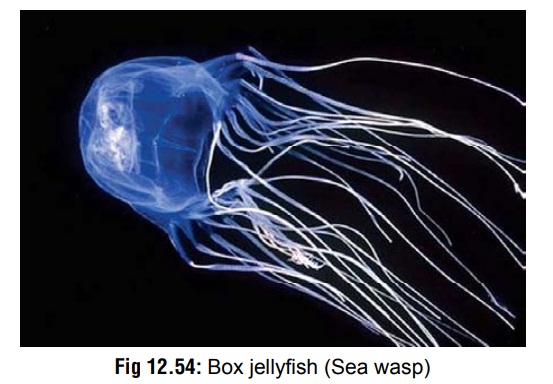
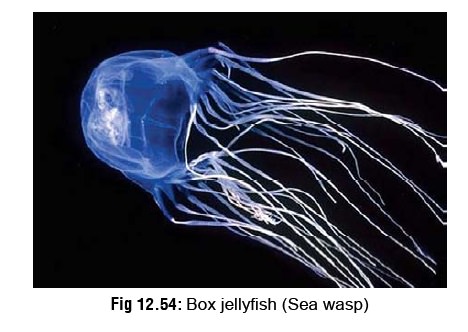
The
box jellyfish, fire medusa, or sea wasp (Chironexfleckeri)
(Fig 12.54) is the most venomous of
all stinging marinecreatures. It has a transparent box- like bell with four
pedalia (feet). Each pedalia may have up to 15 tentacles attached. Because of
its transparency, the box jellyfish is virtually invis-ible under natural
conditions, including clear, sunlit seawater. When fully grown, the bell of Chironex fleckeri may measure up to 30
centimetres in diameter, weigh up to 6 kilograms, and the total length of its
tentacles may be greater than 60 metres. Chironex
fleckeri is predominantly found in northern Australian waters. Each box
jellyfish carries enough venom to kill several adults. Features include
profound muscle spasm, hypotension, acute respiratory distress, respiratory
paralysis, cyanosis, haemolysis, arrhythmias, and cardiac arrest. Severe
parasympathetic dysfunction (abdominal distension, urinary retention, dry eyes)
is common. Death can occur in less than a minute. A few cases have been
reported from India also. Neuromuscular paralysis leading to respiratory arrest
may occur following Chironex fleckeri
stings. The sting of a chirodropid is characteristic for leaving a
“cross-hatched” or “frosted-ladder” tentacle imprint on the skin, as well as
multiple wheals. The skin may become blackened, and permanent scarring may
result.
General Treatment Measures for Cnidarian Stings
·
Anaphylaxis to jellyfish sting must
be treated by main-taining airway and cardiovascular status. Adrenaline is
administered in the usual way. Verapamil may be useful for arrhythmias.
Antihistamines with or without inhaled beta agonists, and corticosteroids may
be required. Topical corticosteroids and oral antihistamines are indicated in
delayed hypersensitivity reactions.
·
Remove any adhering tentacles
carefully without too much tactile pressure which may cause additional
nematocyst discharge. Do not rub the affected area.
·
Inactivate unexploded nematocysts by
topical application of any of the following solutions for at least half an
hour:
o
Vinegar (3 to 5% acetic acid).
Altering pH below 6 inactivates the venom.
o
A slurry (50% w/u) of sodium bicarbonate or baking soda.
Altering pH above 8 dissolves tentacles.
o
Aluminium subacetate 10 to 20% (Burow’s solution). The
aluminium ion denatures protein constituents of venom. Adding 5% detergent
enhances efficacy.
o
Meat tenderiser (papain). It causes denaturation of protein
constituents, but is not as effective as aluminium subacetate.
·
Apply dry baking soda, flour, sand, or shaving soap to the
affected area.
·
Scrape off remaining nematocysts from the wound with a
knife.
·
Wash the area with seawater: Bathe the affected part
liberally with seawater. Do not use fresh or hot water, or alcohol. Fresh
water/alcohol may discharge nematocysts and therefore should be avoided.
·
Apply a steroid cream or lotion (e.g. triamcinolone 0.1%).
If the lesion ulcerates, clean daily with Burow’s solution and cover with dry
dressings.
·
Administer tetanus prophylaxis.
·
For pain: Apply ice-packs for
initial pain relief combined with IV or IM analgesics, if necessary (1 mg/kg of
pethi-dine up to 50 mg, or morphine, 0.1 mg/kg up to 5 mg; can be repeated).
·
Painful muscle spasms may be
relieved by calcium gluco-nate 10% IV.
·
For hypotension: Infuse 10 to 20
ml/kg of isotonic fluid and place in Trendelenburg position. If hypotension
persists, administer dopamine or noradrenaline. Institute central venous
pressure monitoring to guide further fluid therapy.
·
For box jellyfish envenomation,
specific antivenom is available (Commonwealth Serum Laboratories, Melbourne,
Australia). It should be given in life-threatening stings, or severe stings
where the pain is not controlled by other methods. The antivenom should
preferably be given within 4 to 6 hours.
Related Topics