Chapter: Basic Radiology : Brain and Its Coverings
Exercise: Head Trauma
EXERCISE 12-5.
HEAD TRAUMA
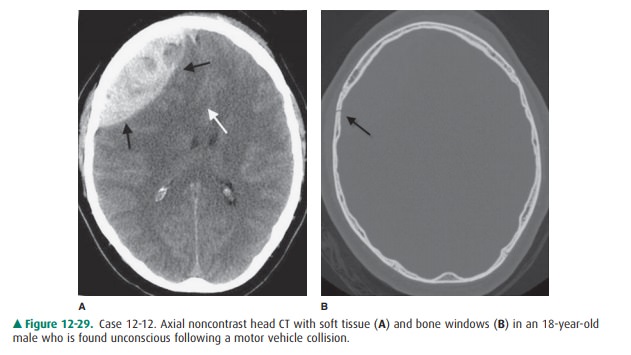
12-12. In Case 12-12, what is the diagnosis (Figure 12-29 A, B)?
A.
Subdural hematoma
B.
Cerebral contusion
C.
Epidural hematoma
D.
Meningioma
E.
Subdural hygroma
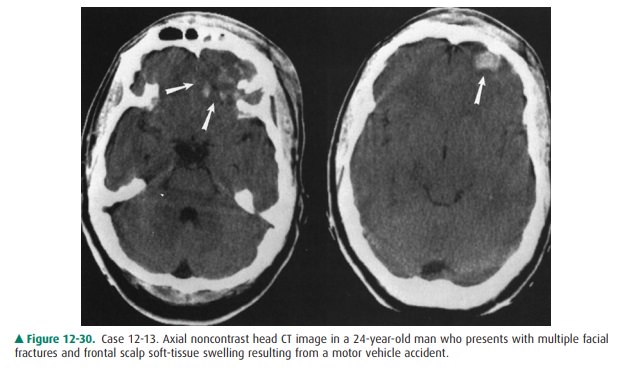
12-13. In Case 12-13, what is the main radiologic finding
(Figure 12-30)?
A.
Subdural hematoma
B.
Epidural hematoma
C.
Duret hemorrhage
D.
Cerebral contusions
E.
Shearing injuries
Radiologic Findings
12-1. In this case, a predominantly
high-density, extra-axial, hemorrhagic collection (black arrows) is pro-ducing
mass effect on the right frontal lobe on an unenhanced head CT scan (Figure
12-29 A). Mass effect results in marked distortion of the underly-ing cortex
and leftward subfalcine herniation (white arrow) (Figure 12-29 A). A linear
nonde-pressed fracture is present along the anterior aspect of the right
parietal bone (black arrow) (Figure 12-29 B). The biconvex appearance of this
lesion is typical of an epidural hematoma, which is the acute finding in this
case (C is the correct answer to Question 12-12).
12-13. In this case, there are multiple
areas of increased at-tenuation within the frontal lobes, especially on the
left (arrows) (Figure 12-30). These areas correspond to multiple hemorrhagic
contusions involving the brain parenchyma (D is the correct answer to Ques-tion
12-13).
Discussion
Intracranial abnormalities in
head trauma can be classi-fied as either primary or secondary. Primary lesions
occur at the moment of injury and include skull fractures, extracerebral
hemorrhage (eg, epidural or subdural hematomas, subarachnoid hemorrhage), and
intracere-bral hemorrhage (eg, brain contusion, brainstem injury, diffuse
axonal injury).
The secondary effects of head
trauma are actually com-plications of the primary intracranial injury. Elevated
in-tracranial pressure and cerebral herniation are responsible for most of the
secondary effects of head trauma, which in many cases may be more devastating
to the patients than the initial injury.
Epidural hematoma is usually
associated with skull fractures that lacerate the middle meningeal artery or a
dural sinus. Up to one-half of patients with epidural hematomas have a lucid
in-terval after the head trauma occurs. On CT, epidural hematomas usually
appear as biconvex, high-attenuation, extra-axial masses. Most are located in
the temporoparietal area. Underlying skull fractures are common. Intracranial
brain herniation may also be a prominent feature in this con-dition. One
important imaging feature in epidural hematomas is that they do not cross skull
sutures, but may cross the midline.
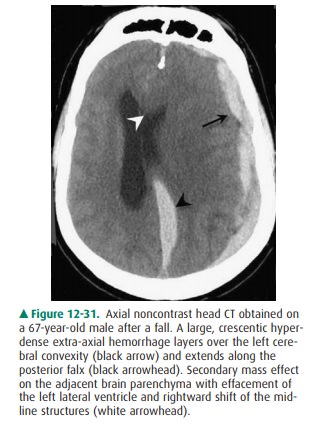
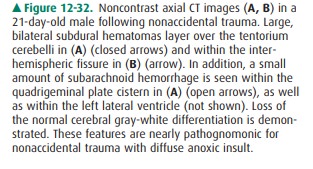
Subdural hematoma, on the other
hand, is usually a cres-cent-shaped extra-axial collection that may cross
suture lines, but is confined by the dural reflections (Figure 12-31). These
lesions are more lethal than are epidural hematomas; the subdural hematoma
mortality rate is over 50%. CT can usually, but not always, distinguish between
epidural hematomas and subdural hematomas. Subdural hematomas are a commonly identified
abnormality in the abused child (nonaccidental trauma). CT scans are obtained
to detect thepresence of subdural hematomas (Figure 12-32). A brain MRI,
however, can more sensitively delineate small extra-axial hematomas, subdural
hematomas of varying ages, and coexisting cortical contusions or shearing
injuries. A shear-ing injury (or diffuse axonal injury) is associated with an
overall poor prognosis and is recognized as small petechial hemorrhages at the
gray-white junction and in the corpus callosum. Interhemispheric (para- and
intrafalcial) sub-dural hematomas may arise from tearing of bridging veins
along the falx cerebri in shaking injuries and are nearly pathognomic for
nonaccidental trauma. Retinal hemor-rhages may be present and are also suspicious,
especially if bilateral. In addition, cerebral ischemia/infarction and
mul-tiple, complex, unexplained skull fractures may be associ-ated findings.
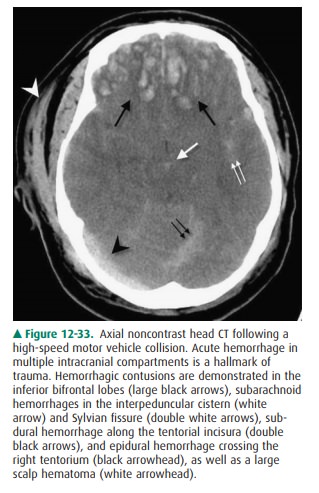
Cerebral contusions (Case 12-13)
are the second most common form of brain parenchymal injury in primary head
trauma (diffuse axonal injury is the most common parenchy-mal injury). Cerebral
contusions can be thought of as brain bruises. They result either from the
brain striking a bony ridge inside the skull during rapid
acceleration/deceleration, as occurs in a motor vehicle accident, or from a
depressed skull fracture. These lesions tend to occur in particular anatomic
locations, especially the undersurfaces and poles of the frontal and temporal
lobes (Figure 12-33). CT scans show areas of low attenuation (edema) and
hemorrhage at the site of injury. Delayed hemorrhage, 1 to 2 days after a head
injury, is common with contusions.
Related Topics