Chapter: Clinical Cases in Anesthesia : Ambulatory Surgery
What sedatives can be administered to supplement a regional anesthetic?
What sedatives can be
administered to supplement a regional anesthetic?
The best anxiolytic may be a solid relationship
between the anesthesiologist and patient; however, excellent rap-port may be
difficult to establish within the confines of a fast-paced ambulatory surgery
center. It has been shown that a preoperative visit with the anesthesiologist
immedi-ately before surgery may serve as a powerful anxiolytic itself.
In the pharmacologic realm, intravenous
midazolam has proven to have excellent sedative and anxiolytic prop-erties
(Table 77.1). It is water-soluble, nonirritating to veins, painless on
administration, provides superb amnesia with rapid onset, and it is therefore
well accepted by patients. Diazepam can cause significant discomfort on
intravenous infusion, and if patients are followed for a number of days after
injection it has been shown to cause thrombophlebitis in a significant number
of cases. Therefore, intravenous diazepam has been virtually elimi-nated from
the practice of anesthesia. Compared with diazepam, midazolam’s much shorter
elimination half-life of 1–4 hours provides a significantly shorter time to
recovery. Midazolam is best titrated every 2 minutes in 1- to 2-mg increments,
because its onset is rapid and effects may be profound. Sedation after
small-to-moderate intravenous doses usually lasts approximately 20–30 minutes.
The pro-found amnestic properties may interfere with assimilating and following
instructions, and patients may become unable to cooperate during surgery. Some
patients who receive the drug may become completely disoriented, uncooperative,
or even combative. This may necessitate either increasing the depth of
sedation, pharmacologic reversal, or conver-sion to a general anesthetic.
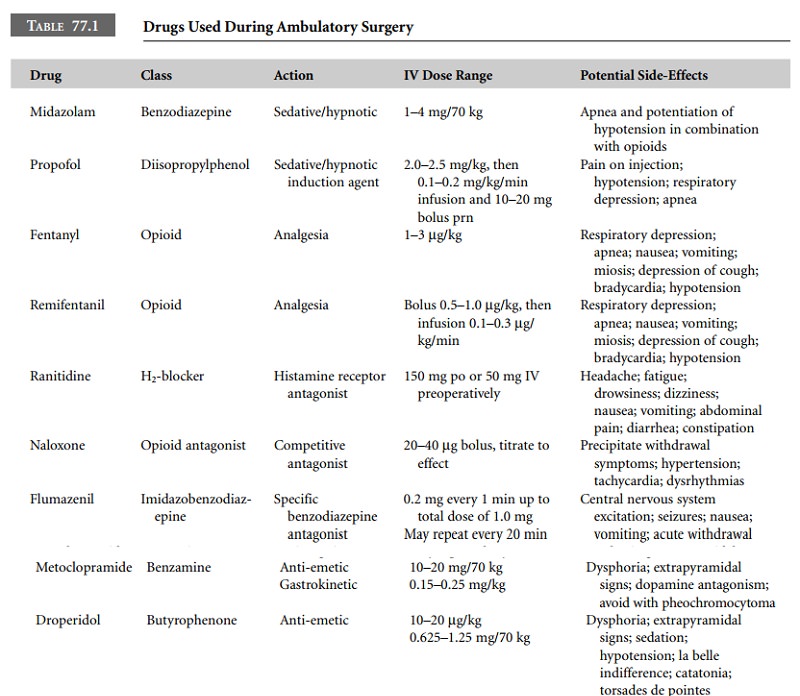
Remifentanil is an excellent addition for the
patient who requires a short-acting opioid to provide analgesia either during
the performance of a painful block or to provide adjunctive analgesia during an
inadequate block. It can be administered by intravenous bolus or by continuous
infusion. Bolus doses of 0.5 μg/kg may be administered with repeat doses
titrated to desired effect. For a continuous infusion, the dose ranges from
0.02 to 0.3 μg/kg/min. Side-effects common to all drugs in the opioid class
include nau-sea, vomiting, and the potential for significant respiratory
depression. Alternatively, fentanyl administered in intra-venous bolus doses of
25–50 μg can be employed to provide adjunctive analgesia. Instead of using
a benzodiazepine to provide sedation, propofol can be administered by either
bolus dose (10–20 mg) or continuous infusion (0.1–0.2 mg/kg/min) and titrated
to the desired hypnotic effect. Inherent anti-nausea and anti-emetic properties
of propo-fol provide a significant advantage in the ambulatory setting.
Related Topics