Chapter: Clinical Cases in Anesthesia : Ambulatory Surgery
What discharge criteria must be met before a patient may leave the ambulatory surgery center?
What discharge criteria must
be met before a patient may leave the ambulatory surgery center?
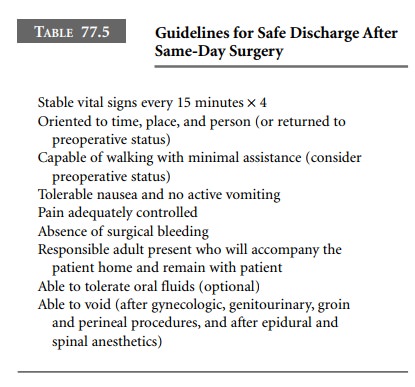
Most institutions divide postanesthesia care
into two phases. The first phase begins when the patient first enters the
recovery area. The second phase, or step-down phase, begins after stability of
vital signs has been achieved and the major effects of anesthesia have
dissipated. At this point, the patient can be comfortably transferred into a
recliner chair, either in the same area or in another unit (Table 77.5).
Patients who have received a spinal or epidural
anes-thetic can only be discharged when full motor, sensory, and sympathetic
function has returned. An inpatient who will remain at bed rest might be
discharged from the PACU to the nursing unit while minimal residual neural
blockade persists; in the case of the ambulatory patient, however, it is
essential that the block has completely dissipated.
Following administration of an epidural or
spinal anes-thetic, the patient should demonstrate the ability to void. This
provides evidence that residual sympathetic blockade has dissipated. Of course,
before attempting to ambulate a patient, it is essential to ensure that all
motor block has resolved.
Patients who have received an ankle block,
brachial plexus block, or peripheral nerve block may be discharged despite the
persistence of residual anesthesia or paresthesias. The arm or foot should be
protected from harm with either a sling in the case of the arm or a bulky
dressing in the case of the foot. The patient needs to be reminded that in time
the block will dissipate and discomfort will appear. For this reason,
instructions should be given to take the prescribed oral analgesic medication
at the first sign of discomfort, because pain is most readily treated before it
becomes excruciating.
Patients who have received general anesthesia
may awaken either in the operating room or shortly after trans-fer to the PACU.
Although the patient may appear to be lucid and oriented, numerous criteria
must be satisfied before a patient may be considered to be ready for discharge
from the facility. A restoration of vital signs within 15–20% of the
preoperative baseline is ordinarily required. Patients should demonstrate an
intact gag reflex and the ability to cough effectively and swallow liquids
without difficulty. It is not necessary for patients to eat before discharge.
Forcing patients to ingest unwanted food in the absence of hunger may simply
serve to increase the incidence of postoperative nausea and vomiting.
Ordinarily, the patient is asked to demonstrate the ability to tolerate a small
amount of liquid. If a patient experiences mild nausea and has not been able to
ingest more than a few sips without precipitating vomit-ing or increased
nausea, it is foolish to persist. Discharge can still be considered, but
written instructions must be provided regarding steps to be taken (contact
facility or surgeon) if there is continued inability to tolerate fluids. It is
important to ensure that a normal state of hydration has been achieved before
discharge. This is especially important following surgery in the oral cavity,
where postoperative pain may preclude early oral intake.
Unless the patient was previously unable to
walk or the procedure performed precludes ambulation, patients should be able
to walk with assistance and without experiencing dizziness. If crutches are
required, it should not be assumed that the patient received preoperative
instruction. Additional instruction should be offered. Hemostasis should be
present at the surgical site, and control of pain should be satisfactory. The
preoperative level of orientation should be achieved, although a mild degree of
residual sedation is acceptable.
It is not essential for a patient to
demonstrate the ability to urinate unless genitourinary, gynecologic, or other
surgery has been performed in the inguinal or perineal region. The patient and
the escort should be instructed of the need to contact either the ambulatory
facility or the surgeon if the patient has not voided within 6 hours following
discharge from the recovery area.
Postanesthesia discharge scoring systems have
been pro-posed and developed for the purpose of assessing when home readiness
is achieved in the postoperative period. Criteria such as mental status, pain
intensity, ability to ambu-late, and stability of vital signs are given numeric
values. A total score above a particular number may indicate a high likelihood
of readiness for discharge. To be practical, a scor-ing system must be readily
understood, simple to employ, and objective. Sophisticated pen-and-paper and
neuro-psychological tests to assess recovery from anesthesia are reserved
solely for research purposes. Actually, after stabil-ity in vital signs is
achieved, the ability of a patient to walk and urinate may be the best measure
of a patient’s gross recovery from an anesthetic and signal readiness for
dis-charge. These activities indicate return of motor strength, central nervous
system functioning, and restoration of sympathetic tone.
Each patient and escort should receive a set of
detailed, written discharge instructions regarding activity, medica-tions, care
of dressings, and bathing restrictions. Instructions must be reviewed verbally
with the patient and escort, and they must be signed by the patient or escort,
if the patient is incapable. Both must be aware of the need to contact the
facility in the event of untoward reac-tions or any difficulties that may arise
such as bleeding, headache, severe pain, or unrelenting nausea or vomiting. The
majority of postoperative complications occur after the patient has been
discharged. Therefore, it is important to ensure comprehension of all
information by the patient or designated escort (Table 77.6).
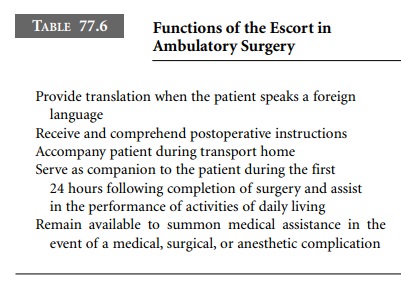
Most states have a mandatory requirement that
patients who have received other than a local anesthetic be dis-charged in the
company of a responsible adult. Current definitions of “responsible adult” vary
and may be broad-ened to include emancipated minors or responsible older
children. Theoretically, the companion should be willing and able to remain
with the patient for at least the first 24 hours after surgery. This is
especially important when deal-ing with the geriatric or debilitated patient.
Problems may arise when an octogenarian patient is discharged in the company of
an octogenarian spouse. Ideally, two adults should accompany pediatric patients
from recovery room to home. After discharge, a child may suddenly experience
nausea or vomiting, pain, fright, or disorientation. A par-ent who is driving a
car cannot possibly attend to both responsibilities simultaneously.
A clear distinction is made between “home
readiness” and “street fitness.” Home readiness signals that the time has
arrived to discharge the patient from the recovery area. On the other hand,
“street fitness” is attained after approximately 24 hours have elapsed, when
most of the more subtle and persistent central nervous system effects of
general anesthesia have dissipated. Patients must be advised not to resume
normal activities immediately upon returning home.
Formal discharge criteria must be in place, and
final evaluations should be conducted immediately before a patient’s discharge
from the unit. All perturbations from normal, including vital signs and unusual
symptoms, must be addressed.
Every attempt must be made to avoid premature
dis-charge of the patient from the PACU. The consequences of such faulty
judgments may include the necessity for emer-gency care elsewhere and possible
readmission to another health care facility. When any element of doubt exists
as to the stability or suitability of a patient for discharge, the better part
of valor is to arrange for hospital admission for overnight observation.
Related Topics