Chapter: Clinical Cases in Anesthesia : Malignant Hyperthermia
What characterizes a clinical episode of MH?
What characterizes a clinical episode of MH?
Typically, an episode is triggered by exposure
to potent inhaled anesthetic agents and/or succinylcholine. The onset time may
be immediate or delayed for as long as 24 hours. Exposure to desflurane
frequently results in a delayed onset of MH. Fulminant MH occurs after a
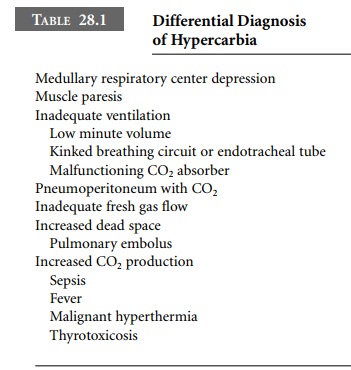
triggering agent causes massive skeletal muscle hyperexcitability. Hypercarbia
man-ifesting as increasing ETCO2 may be the initial sign. Other
causes of hypercarbia are outlined in Table 28.1.
Metabolic acidosis occurs as well and may be
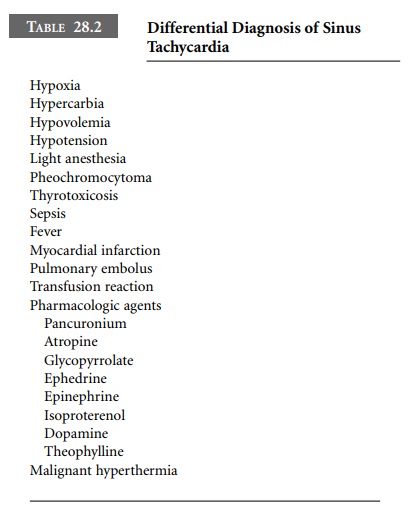
profound. Sympathetic nervous system hyperactivity is demonstrated by
tachycardia and hypertension. The differential diagnosis of sinus tachycardia
is outlined in Table 28.2.
Cardiac dysrhythmias may occur as well.
Elevations of serum potassium, creatine phosphokinase (CPK), myoglo-bin, and
ionized calcium occur as result of increased skele-tal muscle membrane
permeability. Core temperature elevation, potentially exceeding 43°C, is a late
sign. Death may follow. Fulminant episodes involving simultaneous occurrence of
these signs are easily recognizable. Slow evolution of signs demonstrating
certain features, but not others, complicates correct diagnosis.
Confirmation may require detection of myoglobin in the urine. Thyroid
storm, pheochromocytoma, and neurolept malignant syndrome may be difficult to
distinguish from MH.
Related Topics