Chapter: Clinical Cases in Anesthesia : Malignant Hyperthermia
How is MH treated?
How is MH treated?
A suspected case of MH must be treated
promptly, because full-blown episodes proceed rapidly to death.
Triggering agents must be discontinued
immediately. It is no longer recommended that the anesthesia machine be changed
to a “clean” machine (one which has never been used to administer potent
inhaled agents) nor does the breathing circuit have to be changed during an
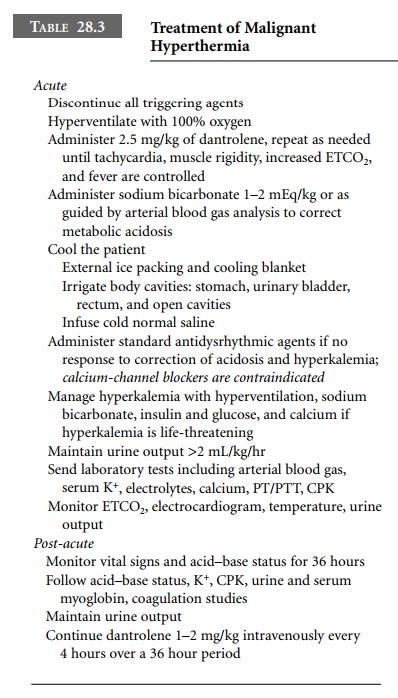
acute episode of MH. Dantrolene is the only drug that effectively treats MH.
Each vial of dantrolene contains 20 mg of dantrolene and 3 g of mannitol, which
must be dissolved in 60 mL of sterile water. The initial dose is 2.5 mg/kg
intra-venously, which may be repeated every 5 minutes until signs abate.
In addition to treating the cause of MH, its
effects must be quickly dealt with. The increase in core temperature must be
treated with cold intravenous fluids, cold irrigation fluids poured into open
body cavities, as well as cold water lavage of the stomach and urinary bladder.
Arterial blood gases should be monitored closely, preferably from an arte-rial
catheter, and the patient should be vigorously ventilated with 100% oxygen to
correct hypercarbia and hypoxemia. Sodium bicarbonate should be used to treat
profound base deficits. Central venous catheters and urinary bladder drainage
catheters help monitor intravascular volume and renal status. Maintaining renal
blood flow is important to prevent renal damage. Intravenous sodium bicarbonate
and acetazolamide alkalinize the urine and prevent precipita-tion of myoglobin
in renal tubules. Diuretics should be given to maintain urine output, and
examination of the urine for myoglobin should be carried out.
Hyperkalemia should be treated with insulin and
50% dextrose solutions, while cardiac dysrhythmias are treated according to
standard protocols. Calcium-channel
blockers are contraindicated because
of their interaction with dantrolene,
possibly resulting in significant hyperkalemia. Following an episode of proven
or suspected MH, the patient should be monitored for 24–36 hours. Recognized
complications of MH include re-emergence, disseminated intravascular
coagulation, and myoglobinuric renal failure. Recommended treatments are given
in Table 28.3.
Related Topics