Chapter: Medicine and surgery: Musculoskeletal system
Systemic sclerosis and scleroderma - Connective tissue disorders
Systemic sclerosis and scleroderma
Definition
Sclerosis (hardening due to excessive production of connective tissue) of collagen affecting the skin (scleroderma) and the internal organs (systemic sclerosis).
Incidence
Rare, 3 per million.
Age
Any age, mean onset at 40 years.
Sex
9F : 1M
Aetiology
Genetic factors are suggested by variations in incidence between ethnic groups and familial clustering.
Infectious and non-infectious environmental agents have also been implicated. A scleroderma like disorder is seen following exposure to silica, vinyl chloride, petroleum-based solvents, rape seed oil and bleomycin.
Pathophysiology
Immune system activation with the production of autoantibodies including antiendothelial cell antibodies and upregulation of cell adhesion molecules causes damage to blood vessels. This results in the release of activating factors, changes in vascular permeability and the proliferation of active fibroblasts, which produce excessive collagen.
Clinical features
A number of patterns of scleroderma and systemic sclerosis are recognised:
Localised scleroderma
Morphoea are patches of sclerotic skin on the trunk and limbs, which may be localised or more generalised.
Linear scleroderma describes a dermatomal distribution of skin and subcutaneous sclerosis.
Systemic sclerosis
Limited cutaneous systemic sclerosis begins with Raynaud’s phenomenon prior to the development of skin sclerosis restricted to the hands (digital ulcers, ischaemia and necrosis), face (beaked nose, small mouth), feet and forearms. Previously this form of systemic sclerosis was referred to as CREST syndrome (calcinosis, Raynaud’s disease, esophageal dysmotility, sclerodactyly andtelangiectasia).
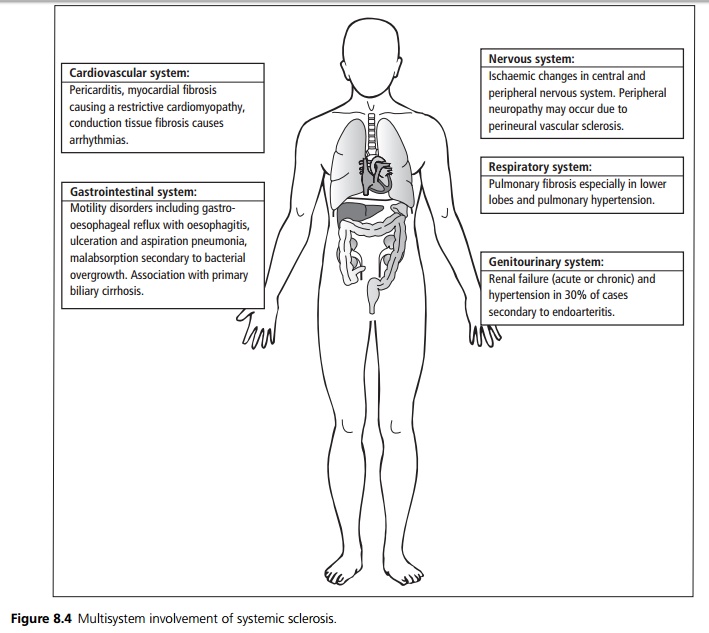
Diffuse cutaneous systemic sclerosis refers to extensive skin sclerosis along with multisystem involvement (see Fig. 8.4).
Systemic sclerosis sine scleroderma is a rare form of the illness in which there is systemic disease in the absence of skin sclerosis.
Overlap syndromes have combinations of the features of systemic sclerosis, systemic lupus erythematosus, dermatomyositis or rheumatoid arthritis.
Microscopy
Extensive deposition of collagen is seen in the skin, viscera, small and medium-sized arteries, arterioles and capillaries. In the wall of blood vessels concentric proliferation and thickening of the intima and fibrosis of the adventitia is seen.
Investigations
As with systemic lupus erythematosus the ESR is raised with a normal CRP.
Autoantibodies include anticentromere, antitopoisomerase-1 (Scl-70), anti-RNA polymerase, and rheumatoid factor is positive in 30%.
Full blood count may show anaemia of chronic disease or haemolytic anaemia.
X-ray changes: In the hands there is a loss of the tufts of the terminal phalanges and soft tissue calcification. There is basal fibrosis in the lungs with reticulonodular shadowing. Contrast imaging of the GI tract may demonstrate oesophageal dilation, poor motility and diverticulae of large bowel.
Management
There is no curative treatment, education is essential and symptomatic treatments initiated.
· Raynaud’s phenomenon is treated by avoiding cold, and vasodilators such as nifedipine, ACE inhibitors or
· in severe cases prostaglandin infusions.
· Oesophageal symptoms are treated with H2 antagonists or proton pump inhibitors, and oesophageal strictures may require repeated dilatation. Malabsorption may require changes in diet.
· Hypertension resulting from renal involvement needs control with ACE inhibitors or calcium channel antagonists.
· The role of immunosuppressive drugs remains unclear.
· Bosentan (an endothelin receptor antagonist) is used in the treatment of pulmonary hypertension secondary to systemic sclerosis and has been shown to reduce the formation of multiple digital ulcers.
Prognosis
Localised forms are milder and do not progress to systemic involvement. No treatment has been shown to alter the long-term progression of scleroderma. Diffuse disease with severe visceral involvement carries the worst prognosis.
Related Topics