Chapter: Essentials of Psychiatry: Personality Disorders
Schizoid Personality Disorder
Schizoid
Personality Disorder
Definition
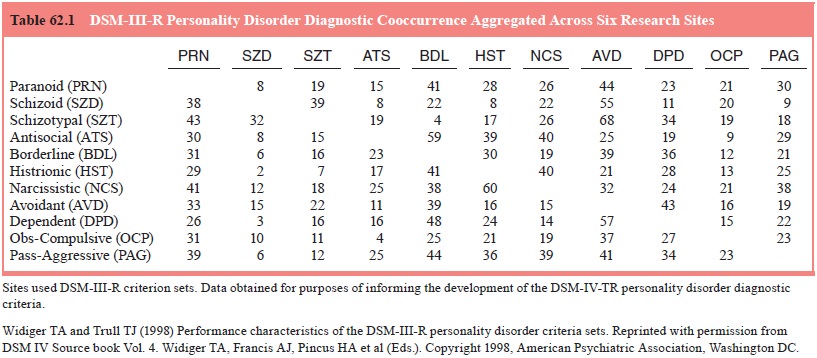
The
schizoid personality disorder (SZPD) is a pervasive pattern of social
detachment and restricted emotional expression. Introver-sion (versus
extraversion) is one of the fundamental dimensions of general personality
functioning. Facets of introversion include low warmth (e.g., cold, detached,
impersonal), low gregarious-ness (socially isolated, withdrawn) and low
positive emotions (reserved, constricted or flat affect, anhedonic), which
define well the central symptoms of SZPD (see Table 62.1). The presence of SZPD
is indicated by four or more of the seven diagnostic criteria presented in the
DSM-IV criteria for SZPD.
Etiology and Pathology
A
fundamental distinction for schizophrenic symptomatology is between positive
and negative symptoms. Positive symptoms include hallucinations, delusions,
inappropriate affect and loose associations; negative symptoms include
flattened affect, alogia, anhedonia and avolition. SZPD has been conceptualized
as rep-resenting subthreshold negative symptoms, comparable to the subthreshold
positive symptoms (cognitive–perceptual aberra-tions) that predominate
schizotypal personality disorder (STPD). However, a genetic link of SZPD to
schizophrenia that cannot be accounted for by comorbid STPD symptomatology has
not been well established. Research has supported heritability for the
personality dimension of introversion–extraversion and for the association of
SZPD with introversion. The central pathology of SZPD does appear to be
anhedonic deficits, or an excessively low ability to experience positive
affect. Psychosocial models for the etiology of SZPD are lacking. It is
possible that a sus-tained history of isolation during infancy and childhood,
with an encouragement and modeling by parental figures of interpersonal withdrawal,
indifference and detachment could contribute to the development of schizoid
personality traits.
Differential Diagnosis
SZPD can
be confused with the schizotypal and avoidant person-ality disorders as both
involve social isolation and withdrawal. Schizotypal personality disorder,
however, also includes an intense social anxiety and cognitive–perceptual
aberrations. The major distinction with avoidant personality disorder is the
absence of an intense desire for intimate social relationships. Avoidant persons
will also exhibit substantial insecurity and inhibition, whereas the schizoid
person is largely indifferent toward the reactions or opin-ions of others.
The
presence of premorbid schizoid traits can have prog-nostic significance for the
course and treatment of schizophrenia but, more importantly, it might not be
meaningful to suggest that a person has a schizoid personality disorder that is
independent of or unrelated to a comorbid schizophrenia. The negative,
pro-dromal and residual symptoms of schizophrenia resemble closely the features
of SZPD. Once a person develops schizophrenia, a diagnosis of SZPD can become
rather pointless as all of the schiz-oid symptoms can then be understood as
(prodromal or residual) symptoms of schizophrenia.
Epidemiology and Comorbidity
Approximately
half of the general population will exhibit an introversion within the normal
range of functioning. However, only a small minority of the population would be
diagnosed with a schizoid personality disorder. Estimates of the prevalence of
SZPD within the general population have been less than 1% and SZPD is among the
least frequently diagnosed personality disor-ders within clinical settings.
Many of the persons who were diag-nosed with SZPD prior to DSM-III are probably
now diagnosed with either the avoidant or the schizotypal personality disorders
and prototypic (pure) cases of SZPD are likely to be quite rare within the
population.
Course
Persons
with SZPD are socially isolated and withdrawn as chil-dren. They may not have
been accepted well by their peers, and may have even borne the brunt of some
ostracism (American Psychiatric Association, 2000). As adults, they have few
friend-ships. The friendships that do occur are likely to be initiated by their
peers or colleagues. They have few sexual relationships and may never marry.
Relationships fail to the extent to which the other person desires or needs
emotional support, warmth and intimacy. Persons with SZPD may do well and even
excel within an occupation, as long as substantial social interaction is not
required. They prefer to work in isolation. They may eventu-ally find
employment and a relationship that is relatively com-fortable, but they could
also drift from one job to another and remain isolated throughout much of their
life. If they do eventu-ally become a parent, they have considerable difficulty
providing warmth and emotional support, and they may appear neglectful,
detached and disinterested.
Treatment
Prototypic
cases of SZPD rarely present for treatment, whether it is for their schizoid
traits or a concomitant Axis I disorder. They feel little need for treatment,
as their isolation is often egosyn-tonic. Their social isolation is of more
concern to their relatives, colleagues, or friends than to themselves. Their
disinterest in and withdrawal from intimate or intense interpersonal contact is
also a substantial barrier to treatment. They at times appear depressed but one
must be careful not to confuse their anhedonic detach-ment, withdrawal and flat
affect with symptoms of depression.
If
persons with SZPD are seen for treatment for a concomi-tant Axis I disorder
(e.g., a sexual arousal disorder or a substance dependence) it is advisable to
work within the confines and limi-tations of the schizoid personality traits.
Charismatic, engaging, emotional, or intimate therapists can be very
uncomfortable, for-eign and even threatening to persons with SZPD. A more
busi-ness-like approach can be more successful.
It is
also important not to presume that persons with SZPD are simply inhibited, shy,
or insecure. Such persons are more appropriately diagnosed with the avoidant
personality disorder. Persons with SZPD are perhaps best treated with a
supportive psychotherapy that emphasizes education and feedback concern-ing interpersonal
skills and communication. One may not be able to increase the desire for social
involvements but one can increase the ability to relate to, communicate with
and get along with others. Persons with SZPD may not want to develop intimate
relationships but they will often want to interact and relate more effectively
and comfortably with others. The use of role playing and videotaped
interactions can at times be useful in this respect. Persons with SZPD can have
tremendous difficulty understand-ing how they are perceived by others or how
their behavior is unresponsive to and perceived as rejecting by others.
Group
therapy is often useful as a setting in which the patient can gradually develop
self-disclosure, experience the interest of oth-ers, and practice social
interactions with immediate and supportivefeedback. However, persons with SZPD
are prone to being rejected by a group due to their detachment, flat affect and
indifference to the feelings of others. If the group is patient and accepting,
they can benefit from the experience.
There
have been many studies on the pharmacologic treat-ment of the schizotypal PD
but no comparable studies on SZPD. The schizotypal and schizoid PDs share many
features, but the responsivity of the schizotypal PD to pharmacotherapy will
usu-ally reflect schizotypal social anxiety and cognitive–perceptual
aberrations that are not seen in prototypic, pure cases of SZPD.
Related Topics