Chapter: Surgical Pathology Dissection : The Female Genital System
Radical Hysterectomy for Cervical Cancer
Radical Hysterectomy for Cervical Cancer
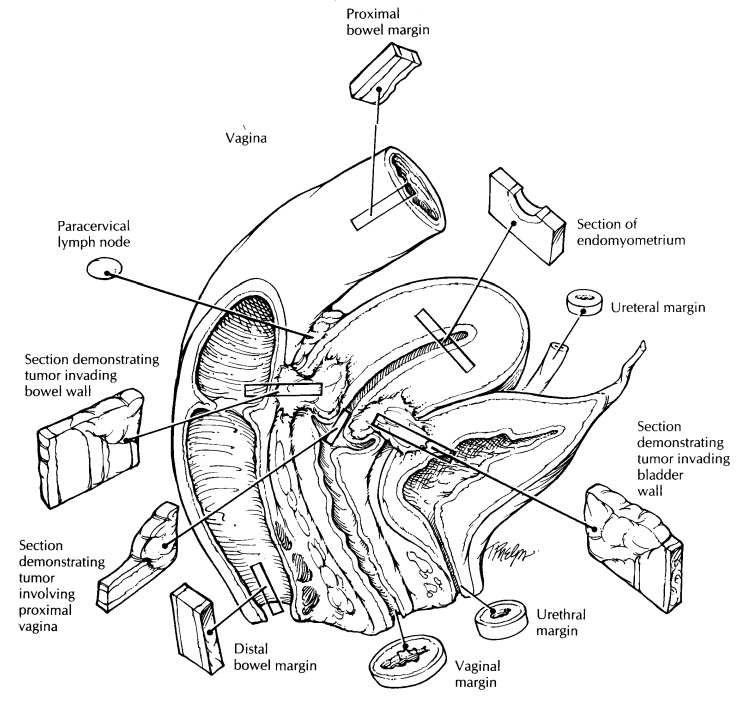
Radical hysterectomies are performed for early stage invasive squamous carcinomas and adenocarcinomas of the cervix. In addition to the uterus and cervix, the specimen has attached para-metrial/paracervical soft tissue and a vaginal cuff.
Begin by
orienting, measuring, and weighing the uterus and cervix as described in the
section on hysterectomies for benign disease. Also, mea-sure the size of the
attached parametrial/paracer-vical tissue and the length of the attached
vaginal cuff. Note whether the shape of the cervix is rounded or barrel shaped.
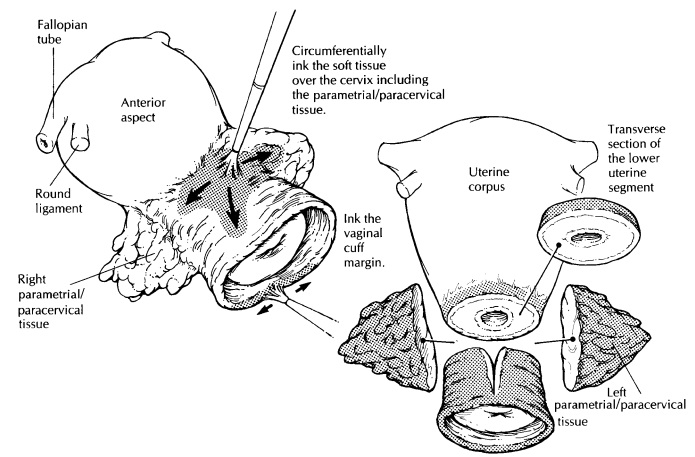
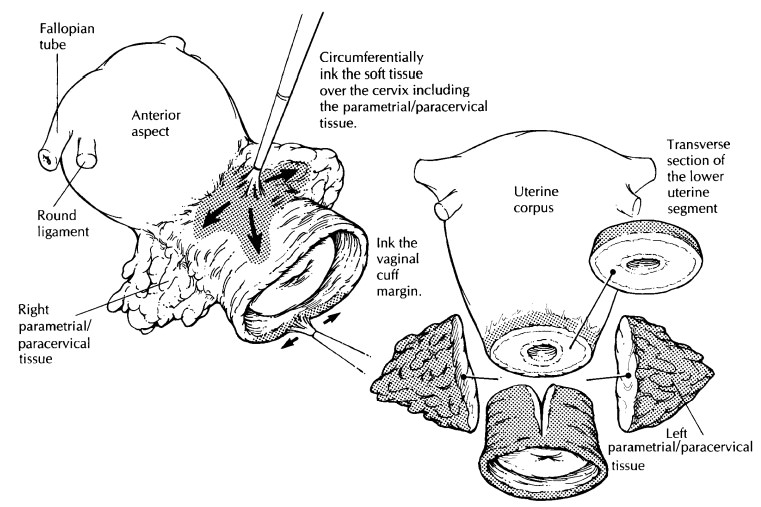
Ink the right and left parametrial/paracervical tissues, the anterior/
posterior soft tissue margins of the cervical canal, and the vaginal cuff
margin. Remove the para-metrial/paracervical tissue by shaving each side close
to its lateral attachment on the cervix. Sec-tion this tissue at 0.3-cm
intervals, and submit the entire tissue for histologic examination. Any
identifiable lymph nodes may be dissected and separately designated.
Next,
amputate the cervix at the level of the internal os, and open the canal with a
longitudi-nal incision opposite the tumor. Pin it open, and fix it as you would
a cone biopsy. Measure the maximum tumor width and length as well as the
distance to the nearest vaginal margin. Exam-ine the vaginal cuff. Unless the
tumor is close to the vaginal margin, the margin may be removed with a 0.3-cm
parallel shave and submitted as four designated quadrants. If the tumor closely
approaches the vaginal margin, leave the vaginal cuff intact and take
perpendicular margins to demonstrate the relationship of the tumor to the
margin. Serially section the cervix at 0.3-cm inter-vals, and measure the
maximum tumor thickness as well as the thickness of the cervical wall at that
site. Occasionally, a cervical tumor may not be easily discernible as a result
of prior surgery or therapy.
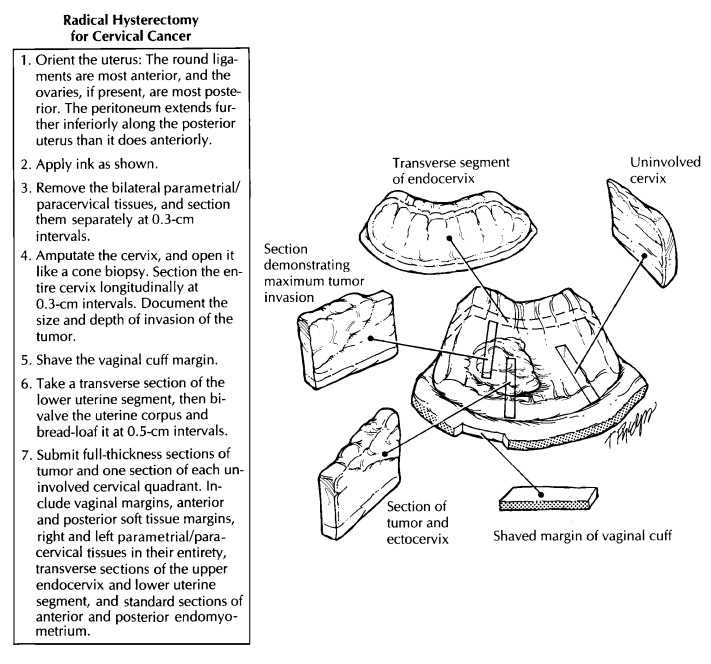
Now turn
your attention to the uterine corpus. Take a transverse section of the lower
uterine segment and bivalve the uterus into anterior and posterior halves.
Examine the corpus with serial transverse sections as you would in any hysterec-tomy
specimen.
Sections
for microscopic analysis should be chosen to demonstrate the maximum thickness
of the tumor and its interface with any normal-appearing mucosa. If the tumor
is not visible, the cervix with attached vaginal cuff should be entirely
submitted as in a cone biopsy. The su-perior extent of the tumor can be
documented by taking transverse sections of the upper endo-cervix and lower
uterine segment. The inferior extent of the tumor is documented by taking
sections of the cervical tumor that include the adjacent vaginal tissue.
Margins to be evaluated include the left and right parametrial/paracervi-cal
tissues, submitted in their entirety, and the vaginal cuff. The anterior and
posterior cervical soft tissue margins should be submitted to de-lineate the
extent of the tumor in relationship to the bladder and rectum.
![]()
Lymph
nodes are usually submitted separately by the surgeon from the right and left
internal iliac, external iliac, obturator, pelvic, and para-aortic node groups.
They can be handled in a routine manner for evaluation of metastatic disease.
Important Issues to Address in Your Surgical Pathology Report on Radical Hysterectomies for Cervical Cancer
· What
procedure was performed, and what structures/organs are present?
· What are
the histologic type and grade of the tumor?
· Are any
associated precursor lesions present [cervical intraepithelial neoplasia (CIN)
or ade-nocarcinoma in situ (AIS)]?
· What is
the tumor size? Give horizontal spread (in millimeters) for microinvasive tumors
and overall size (in centimeters) for gross tu-mors. State which quadrants of
the cervix are involved.
· What is
the maximum depth of invasion (in millimeters)? Measure from the base of the
squamous or glandular epithelium from which it originates.
· What is
the thickness of the cervical wall at the point of deepest tumor invasion (in
milli-meters)?
· Does the
tumor involve capillary–lymphatic spaces?
· Does the
tumor extend into the vagina, para-metrial/paracervical tissue, uterus, or
adnexa? Specify the extent of involvement and depth of invasion.
· Does the tumor involve any resection margins (vaginal, anterior and posterior cervical, and bi-lateral parametrial/paracervical)? If the tumor is close to but does not involve a resection
·
margin, give the distance between the tumor and
the margin (in millimeters).
·
Is metastatic disease present? Record the
num-ber of lymph nodes with metastases and the number of lymph nodes identified
by site.
Related Topics