Chapter: Psychology: Memory
Psychology: Explicit and Implicit Memory
Explicit and
Implicit Memory
We’ve now considered several ways
that explicit memory might be subdivided—into episodic memory and semantic, and
then with each of those categories potentially divided further. But what about implicit memory? As we’ll see, this
memory provides an entirely different means through which we’re influenced by
past experience, and it is distinct from explicit memory in its functioning and
in its biological basis.
DISTINGUISHING IMPLICIT FROM EXPLICIT MEMORY
Implicit memories are
distinguishable from explicit memories in many ways. Perhaps the clearest
evidence, however, comes from the study of the memory disruption caused by
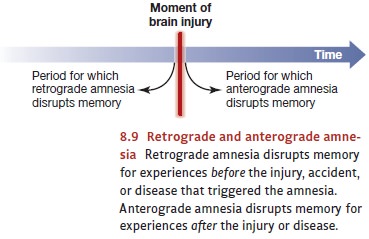
brain damage. In general, this disruption is referred to as amnesia. Earlier, we mentioned one type
of amnesia: retrograde amnesia—a loss
of memories for events that took place before the brain injury that caused the
amnesia. In other cases, though, brain damage produces anterograde amnesia—an apparent inability to form new memories (see
Figure 8.9).
In general, anterograde amnesia
is caused by damage to certain sites in the temporal cortex—specifically, in
the hippocampus and nearby subcortical regions. In some cases, this damage is
the result of illness—especially if the illness causes encephalitis, an inflammation in the brain tissue. In other cases,
the damage is caused by stroke or physical trauma. One of the most common
causes, though, is a type of malnutrition associated with chronic alcoholism;
in this case, the amnesia is a central symptom of the illness called Korsakoff ’s syndrome.
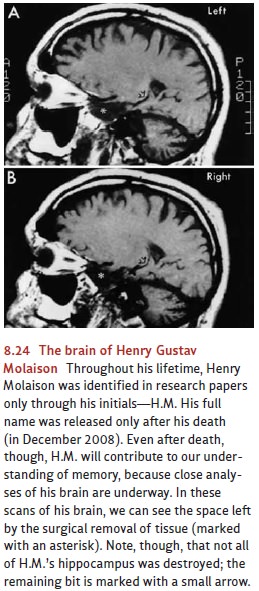
One of the most carefully studied
cases of anterograde amnesia, however, had an entirely different cause: A
patient known as H.M. suffered from severe epilepsy. When all other treatments
failed, the physicians tried (in the late 1950s) to treat H.M.’s disease with a
neurosurgical procedure that deliberately removed most of his hippocampus,
amygdala, and a considerable amount of nearby tissue (Figure 8.24). The
procedure was, in a very narrow sense, a success: It did control his epilepsy.
But the surgery also had a tragic and unanticipated side effect. Across the 55
years he lived after his surgery, H.M. seemed incapable of adding new
information to his long-term memory. As his obituary put it: “each time he met
a friend, each time he ate a meal, each time he walked in the woods, it was as
if for the first time” (Carey, 2008). He remembered none of the episodes in his
life after the surgery; he was entirely unable to recognize people he’d first
met after the surgery—even if he saw them day after day (Milner, 1966, 1970;
also see O’Kane, Kensinger, & Corkin, 2004; Skotko et al., 2004).
Amnesia had devastating effects
on H.M.’s life—including some effects that we might not think of as involving
memory. For example, H.M. had an uncle he liked very much. When first told that
his uncle had died, he was deeply distressed, but then he for-got all about
this sad news. Some time later, he asked again when his uncle would come to
visit, and he was told again of his uncle’s death. His grief was as intense as
before; indeed, each time he heard this sad news, he was hearing it for the
first time—with all the shock and pain (Corkin, 1984; Hilts, 1995;
Marslen-Wilson & Teuber, 1975; Milner, 1966; Milner, Corkin, & Teuber,
1968).
Crucially, and despite these
remarkable problems, patients with anterograde amnesia— including H.M.—can
acquire certain types of new memories which can be revealed with specialized
testing. In some studies, for example, patients with anterograde amnesia have
been given practice, day after day, in finding the correct path through a maze.
Each time they’re shown the maze, the patients insist they’ve never seen it
before; this is simply a con-firmation of their amnesia. Even so, they get
faster and faster in solving the maze—and so apparently they do retain some
information from each practice session.
Likewise, in another study, patients with Korsakoff ’s syndrome heard a series of brief melodies (Johnson, Kim, & Risse, 1985). A short time later, they listened to a new series and were told that some of the tunes in the second batch were repeats from the earlier presentation. As expected, these amnesic patients were completely unable to tell which tunes were the repeats and which were new; indeed, their memory responses were close to random. Remarkably, though, when asked which melodies they preferred, the patients uniformly preferred the familiar ones. The patients had no (explicit) memory for these tunes, but a memory did emerge with indirect testing—and emerged, in this case, as a preference.
In important ways, therefore,
these patients can’t remember their experiences. If we ask them directly about
the past, they recall nothing. If we ask them which mazes they have solved before
and which are novel, they can only guess. Thus it seems clear that these
patients have no conscious recollection, no explicit
memory, for the events in their lives. Still, we can find ways in which the
patients’ current skills and behaviors are shaped by their experiences—and so,
apparently, the experiences have left some record, some residual imprint, in
these patients. This lasting imprint, a demonstrable impact of the past, is
what psychologists call implicit memory—an
unnoticed “leftover” from life events that changes how someone now acts and
thinks (Donaldson, Peterson, & Buckner, 2001; Fazio & Olson, 2003;
Humphreys et al., 2003; Kinoshita, 2001; Yonelinas, 2002).
PROCEDURAL MEMORY
What exactly is implicit memory?
In what circumstances does it influence us? And can implicit memory be
demonstrated in people without amnesia, people whose brains are healthy and
intact? To answer these questions, we need to distinguish different types of
implicit memory, because each type influences us in its own way.
Some cases of implicit memory
involve procedural knowledge rather
than declarative knowledge. Procedural
knowledge is knowinghow—knowing how
to ridea bicycle, for example, or how to use chopsticks. Declarative knowledge,
in contrast, is represented in explicit memory, not implicit, and it’s knowingthat: knowing that there are three outs
in an inning, that automobiles run on gasoline, or that you woke up late this
morning.
The earlier example we mentioned
in our discussion of amnesia—that of patients learning how to get through a
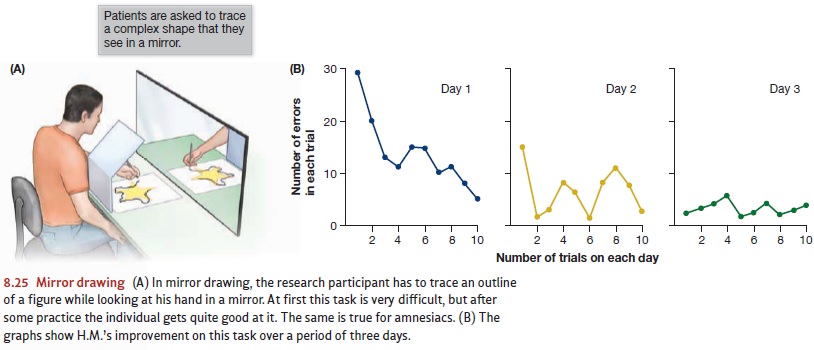
maze—involves procedural memory, and other examples are easy to find. In some
procedures, patients have been shown a complex shape and asked to trace the
outline of the shape with a stylus. What made this task difficult was that the patients
couldn’t see the shape directly; they could see it (and the stylus) only by
looking into a mirror (Figure 8.25). This task is moderately difficult—but the
patients got better with practice, all the while insisting that each try at the
task was their very first time.
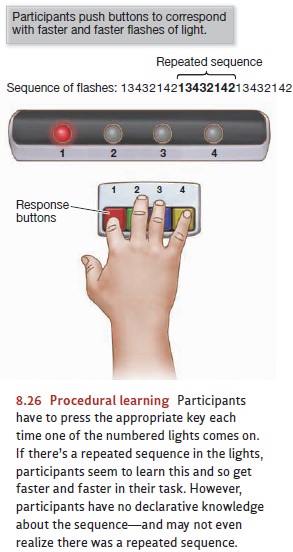
What about people who don’t have
amnesia—people with normal brains? In some studies, research participants are
given four buttons and told to press button 1 if light 1 comes on, button 2 for
light 2, and so on (Figure 8.26). The lights are then turned on in rapid
succession, and participants do their best to keep up. As it turns out, the
lights are turned on in a repetitive sequence—perhaps always
1-3-4-2-1-4-1-3-4-2-1-4-1-3-4-2-1-4. Participants seem to learn this sequence;
and so, with a bit of practice, can respond more quickly if the lights follow
this sequence than they can if the sequence is random. But when asked whether
the sequence was random or not, participants are clueless. Thus, they seem to
have procedural knowledge that allows them to respond more quickly to the
patterned lights, but they don’t have declarative knowledge—the same
distinction we observe in patients with amnesia (Gazzaniga et al., 2009).
PRIMING EFFECTS
Procedural memories are typically
concerned with behaviors—our actions and our skills. Other types of implicit
memory, in contrast, influence our perceptions and our thoughts. Consider, for
example, demonstrations of priming.
Participants in one study were shown a number of words. Later, they were given
a second task in which they sim-ply had to identify words flashed briefly on a
computer screen. Participants had no idea that many of the words in this second
task were taken from the earlier list, but they still showed a pattern known as
repetition priming: Words that had
been on the original list were identified more readily than words that had not.
This priming was observed even for words that the participants failed to
recognize as familiar in a standard recognition task. Thus, the participants
had no explicit memory for having seen these words, but they did have an
implicit memory that showed up as priming. In other words, they were being influenced
by a memory they didn’t realize they had (Jacoby, 1983; Jacoby &
Witherspoon, 1982).
Other procedures, with different
tasks, show a similar pattern. In fragment-completiontasks,
for example, participants are shown partial words (such as C_O_O_I_E)
andasked to complete them to form actual words (CROCODILE). Success in this
task is much more likely if the target word was encountered recently; this
advantage is observed even when participants have no conscious recollection of
the previous encounter (Graf & Mandler, 1984; Jacoby & Dallas, 1981;
Tulving, Schacter, & Stark, 1982).
In another experiment,
participants were asked to read sentences that were pre-sented to them upside
down. A year later, participants
returned to the lab; there, they were shown a series of sentences and asked
which ones they’d seen in their first visit to the lab and which ones were
novel. Not surprisingly, after this long delay, participants couldn’t tell
which sentences they’d seen before. Still, when they were asked once again to
read sentences presented upside down, they were faster with the sentences
they’d seen before than they were with novel sentences—a case of priming that
lasted across a full 12 months (Kolers & Roediger, 1984).
In each of these cases, it seems
that an encounter with a stimulus leaves us better prepared for that stimulus
the next time we meet it. This preparation can then influence us in many ways,
quite independently of whether we can recall the earlier encounter with that
stimulus. To illustrate how far this pattern can reach, consider the so-called
illusion of truth. In the relevant studies, participants hear a series of
statements like “The average person in Switzerland eats about 25 pounds of
cheese each year,” or “Henry Ford forgot to put a reverse gear in his first
automobile.”* Participants’ task is to say how interesting each of these statements is. Later on, the same
participants are presented with some more sentences but now have to rate the
credibility of each one on a scale from “certainly true” to “certainly false.”
Needless to say, some of the sentences in this “truth test” are repeats from
the earlier presentation; the question for us is how the judgments of sentence
credibility are influenced by the earlier exposure.
The result of these studies is a
propagandist’s (or advertiser’s) dream: Sentences heard before are more likely
to be accepted as true, so that in essence familiarity increases credibility
(Begg, Anas, & Farinacci, 1992). To make matters worse, the effect emerges
even when participants are warned not to believe the sentences in the first
list. That is, sentences plainly identified as false when they’re first heard
still create the illu-sion of truth, so that these sentences are subsequently
judged to be more credible than sentences never heard before.
How could this be? Bear in mind
that the participants in these procedures are shown a lot of sentences and that
there’s a delay between the first task (judging how interest-ing the sentences
are) and the second (judging credibility). These steps make it difficult for
participants to keep track of the sentences they hear; in other words, these
steps work against explicit memory. As a result, participants have a hard time
recalling which of the sentences in the truth test they encountered on the
first list; so it doesn’t help them to know that the sentences on that first
list were all false. Thus, with no conscious memory of the earlier encounter,
participants have no way to protect themselves from the illusion.
OTHER FORMS OF
IMPLICIT MEMORY
We’ve now mentioned two forms of
implicit memory—priming effects and procedural memory—but there are other forms
as well. One plausible addition to this list is perceptual learning—the learning that you need to do whenever you
“recalibrate” yourperceptual systems. As an example, think of what happens when
someone gets new eyeglasses, perhaps with a stronger prescription than they’ve
had before. Across the next few days, he needs to “adjust” to the glasses—changing
(among other things) how he interprets the degree of tension in his eye muscles
as a cue to distance. This is surely a form of learning—and so places new
information, or perhaps new skills, in memory. But it’s learning that happens
completely outside of awareness—and so involves implicit memory, not explicit.
A different example involves
cases including the learn-ing called classical
conditioning. This learning, too, creates new knowledge—knowledge about
what follows what in the world—but can be done without conscious awareness.
Indeed, classical conditioning can take place even if an organism is fully
anesthetized during the learning (e.g., Cahoon, 2008).
These and other examples
demonstrate the enormous breadth of implicit memory. We rely on explicit memory in many circumstances,
and we’re guided to an enormous extent by our conscious recollection of the
past. But the reach of implicit memory may be even larger—so that in many
situations, we’re shaped in ways we do not notice by past experiences that we
cannot recall.
Related Topics