Chapter: Clinical Anesthesiology: Anesthetic Equipment & Monitors : Non cardiovascular Monitoring
Precordial & Esophageal Stethoscopes - Respiratory Gas Exchange Monitors
Respiratory Gas Exchange Monitors
PRECORDIAL & ESOPHAGEAL STETHOSCOPES
Indications
Prior to the routine availability of gas
exchange monitors, anesthesiologists used a precordial or esophageal
stethoscope to ensure that the lungs were being ventilated in the event that
the circuit became disconnected. Likewise, the heart tones could be auscultated
to confirm a beating heart. Although less essential today because other
modalities are available, the finger on the pulse and auscultation remain
front-line monitors, especially when tech-nology fails. Chest auscultation
remains the primary method to confirm bilateral lung ventilation in the
operating room, even if end tidal CO 2
detectionis the primary mechanism to exclude esophageal intubation.
Contraindications
Instrumentation of the esophagus should
be avoided in patients with esophageal varices or strictures.
Techniques & Complications
A precordial stethoscope (Wenger
chestpiece) is a heavy, bell-shaped piece of metal placed over the chest or
suprasternal notch. Although its weight tends to maintain its position,
double-sided adhe-sive disks provide an acoustic seal to the patient’s skin.
Various chestpieces are available, but the child size works well for most
patients. The bell is con-nected to the anesthesiologist by extension tubing.
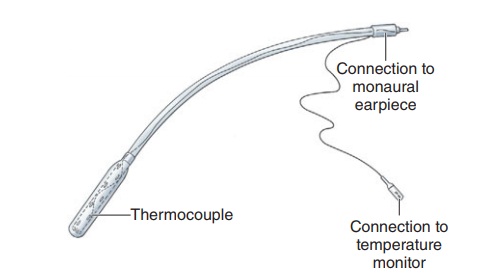
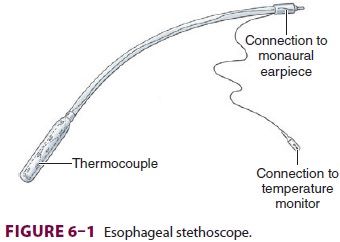
The esophageal stethoscope is a soft plastic
cath-eter (8–24F) with balloon-covered distal openings (Figure 6–1). Although the
quality of breath and heart sounds is much better than with a precordial
stethoscope, its use is limited to intubated patients. Temperature probes,
electrocardiogram (ECG) leads, ultrasound probes, and even atrial pacemaker
electrodes have been incorporated into esophageal stethoscopes. Placement
through the mouth or nose can occasionally cause mucosal irritation and
bleed-ing. Rarely, the stethoscope slides into the trachea
instead of the esophagus, resulting in a
gas leak around the tracheal tube cuff.
Clinical Considerations
The information provided by a precordial
or esoph-ageal stethoscope includes confirmation of ventila-tion, quality of
breath sounds (eg, stridor, wheezing), regularity of heart rate, and quality of
heart tones (muffled tones are associated with decreased cardiac output).The
confirmation of bilateral breath sounds after tracheal intubation, however, is
made with a binaural stethoscope.
Related Topics