Chapter: Clinical Anesthesiology: Anesthetic Equipment & Monitors : Non cardiovascular Monitoring
Cerebral Oximetry and Other Neurological System Monitors of the Brain
CEREBRAL OXIMETRY AND OTHER MONITORS OF THE BRAIN
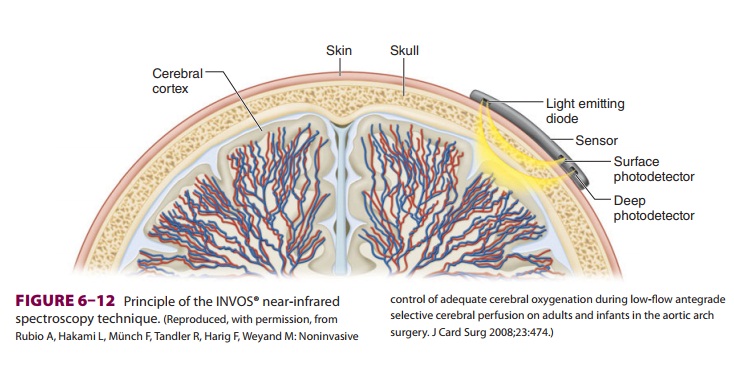
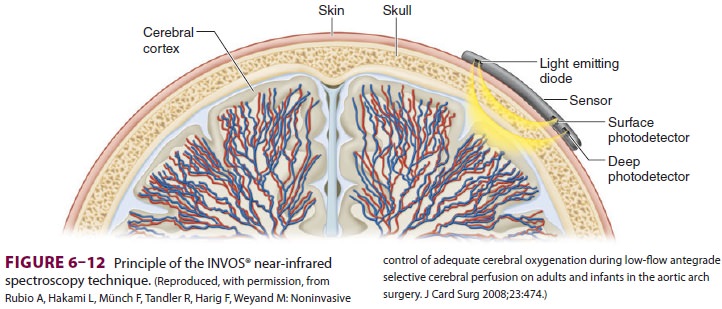
Cerebral oximetry uses near infrared
spectros-copy (NIRS). Using reflectance spectroscopy near infrared light is
emitted by a probe on the scalp (Figure 6–12). Receptors are likewise
positioned to detect the reflected light from both deep and super-ficial
structures. As with pulse oximetry, oxygenated and deoxygenated hemoglobin
absorb light at dif-ferent frequencies. Likewise, cytochrome absorbs infrared
light in the mitochondria. The NIRS satura-tion largely reflects the absorption
of venous hemo-globin, as it does not have the ability to identify the
pulsatile arterial component. Regional saturations of less than 40% on NIRS
measures, or changes of greater than 25% of baseline measures, may herald
neurological events secondary to decreased cerebral oxygenation.Measurements of
jugular venous bulb satura-tion can also provide estimates of cerebral tissue
oxygen extraction/decreased cerebral oxygen deliv-ery. Reduced saturations may
indicate poor out-comes. Direct tissue oxygen monitoring of the brain is
accomplished by placement of a probe to deter-mine the oxygen tension in the
brain tissue. In addi-tion to maintaining a cerebral perfusion pressure that is
greater than 60 mm Hg and an intracranial pressure that is less than 20 mm Hg,
neuroanesthe-siologists/intensivists attempt to preserve brain tis-sue
oxygenation by intervening when oxygen tissue tension is less than 20 mm Hg.
Such interventions center upon improving oxygen delivery by increas-ing Fio2, augmenting hemoglobin, adjusting cardiac output,
or decreasing oxygen demand.
Related Topics