Chapter: Medicine and surgery: Respiratory system
Pneumothorax
Pneumothorax
Definition
Defined as air in the pleural space which may be traumatic or spontaneous.
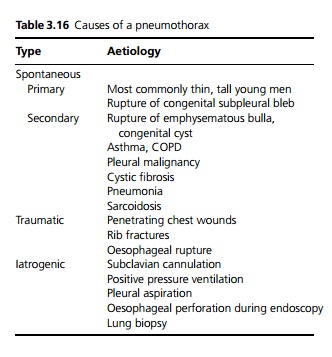
Aetiology
See Table 3.16.
Clinical features
Sudden onset of unilateral pleuritic pain and/or increasing breathlessness is the usual presenting feature. Large pneumothoraces produce breathlessness, pallor, tachycardia and even hypotension. About one third recur.
Investigations
Chest X-ray shows the visceral pleura as a thin line with absent lung markings beyond.
Management
· Observation if the pneumothorax is small. The air is reabsorbed gradually over days to weeks.
· If the pneumothorax is >20%, particularly if the patient has underlying lung disease or is significantly dyspnoeic, then simple aspiration is indicated.
· If this fails, i.e. the lung does not reinflate sufficiently or if the pneumothorax recurs, an intercostal drain with underwater seal is required. If after a few days the drain continues to bubble and the pneumothorax persists this indicates a bronchopleural fistula, i.e. a continued leak of air from the lung to the pleural space. This may require surgical treatment.
· Pleurectomy is indicated in recurrent pneumothoraces or for bronchopleural fistulae that fail to close with conservative management. This is performed by stripping the pleura from the inside of the chest through a limited thoracotomy. Any blebs or bullae are stapled or tied off and the lung reinflated. The opposition of lung to the raw area on the chest wall causes the surfaces to adhere to one another. Talc or another irritant is often used to improve this adherence.
· Tension pneumothorax (a large pneumothorax causing mediastinal shift) is a medical emergency and requires aspiration immediately.
Related Topics