Chapter: Medicine and surgery: Respiratory system
Extrinsic allergic alveolitis - Restrictive lung disorders
Extrinsic allergic alveolitis
Definition
An immune reaction within the lung to inhaled organic dusts.
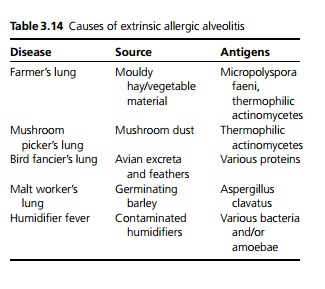
Aetiology
See Table 3.14
Pathophysiology
· After exposure there is formation of antibody–antigen complexes. Normally immune complexes are cleared but if they persist, they activate the complement system resulting in local inflammation, inflammatory cell recruitment and cellular damage (i.e. a type III hypersensitivity reaction).
· If there is repeated exposure a type IV cell mediated hypersensitivity reaction occurs with the formation of small granulomas. The lung damage is repaired by pulmonary fibrosis.
Clinical features
· Fever, malaise, cough and shortness of breath, some-times with limb pains, develops several hours after exposure to the antigen and may last up to 2–3 days. On examination there may be tachypnoea and cyanosis, with widespread fine end-inspiratory crackles and mild wheeze.
· Chronic exposure leads to a chronic disease characterised by weight loss, effort dyspnoea, cough and signs similar to idiopathic pulmonary fibrosis (persisting cyanosis, fine crackles and cor pulmonale).
Microscopy
Infiltration with neutrophils, lymphocytes and macrophages. In chronic exposure non-caseating granulo-mas are seen comprising multinucleated giant cells, within which the antigenic material may be demonstrated.
Complications
Diffuse fibrosis and formation of honeycomb lung in about 5%.
Investigations
Chest X-ray shows a diffuse haze initially, which develops into micronodular shadowing. The upper lobes are predominantly affected. Advanced cases may show features of honeycomb lung (cystic appearance). CT chest shows ground glass appearance in acute forms due to alveolitis and extensive lung fibrosis with nodule formation in chronic cases.
There is a raised white count with a neutrophilia following acute exposure. There is no eosinophilia (this would suggest asthma).
Precipitating antibodies are present in the serum; however, these are markers of exposure and not of the disease.
Respiratory function tests shows a restrictive pattern with reduced lung volumes, FEV1 and FVC are low but the ratio of the two is normal/high, and gas transfer is reduced. This is reversible initially, but becomes permanent with chronic disease.
Bronchoalveolar lavage shows an increase in lymphocytes and macrophages.
Management
1. Avoidance is the most important factor in management, mainly by changing working practice.
2. High-dose prednisolone is used to cause regression of the early stages of the disease, later stages where there is fibrosis are not amenable to treatment.
Prognosis
Recurrent exposure leads to irreversible damage and ultimately respiratory failure, and it is particularly difficult to stop bird fanciers from pursuing their hobby. Farmer’s lung is an occupational disease in the United Kingdom with sufferers being entitled to compensation.
Related Topics