Chapter: Medical Surgical Nursing: Management of Patients With Complications From Heart Disease
Pericardial Effusion and Cardiac Tamponade
PERICARDIAL
EFFUSION AND CARDIAC TAMPONADE
Pathophysiology
Pericardial
effusion refers to the accumulation of fluid in the peri-cardial sac. This
occurrence may accompany pericarditis, advanced HF, metastatic carcinoma,
cardiac surgery, trauma, or nontraumatic hemorrhage.
• Increased right and left ventricular end-diastolic pressures
• Decreased venous return
• Inability of the ventricles to distend adequately and to fill
Pericardial
fluid may accumulate slowly without causing no-ticeable symptoms. A rapidly
developing effusion, however, can stretch the pericardium to its maximum size
and, because of in-creased pericardial pressure, reduce venous return to the
heart and decrease CO. The result is cardiac tamponade (compression of the
heart).
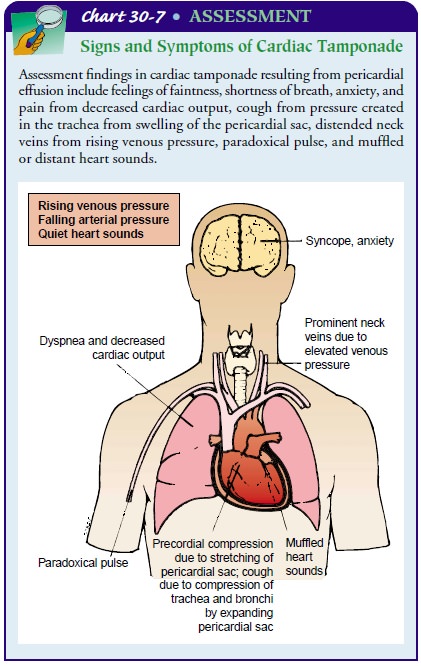
Clinical Manifestations
The
patient may complain of a feeling of fullness within the chest or may have
substantial or ill-defined pain. The feeling of pres-sure in the chest may
result from stretching of the pericardial sac. Because of increased pressure
within the pericardium, venous pressure tends to rise, as evidenced by engorged
neck veins. Other signs include shortness of breath and a drop and fluctuation
in blood pressure. Systolic blood pressure that is detected during ex-halation
but not heard with inhalation is called pulsus
para-doxus. The difference in systolic pressure between the point thatit is
heard during exhalation and the point that it is heard during inhalation is
measured. Pulsus paradoxus exceeding 10 mm Hg is abnormal. The cardinal signs
of cardiac tamponade are falling systolic blood pressure, narrowing pulse
pressure, rising venous pressure (increased jugular venous distention), and
distant (muf-fled) heart sounds (Chart 30-7).
Assessment and Diagnostic Findings
Pericardial
effusion is detected by percussing the chest and notic-ing an extension of
flatness across the anterior aspect of the chest. An echocardiogram may be
performed to confirm the diagnosis. The clinical signs and symptoms and chest
x-ray findings are usu-ally sufficient to diagnose pericardial effusion.
Medical Management
PERICARDIOCENTESIS
If cardiac function becomes seriously impaired, pericardiocen-tesis (puncture of the pericardial sac to aspirate pericardial fluid)is performed to remove fluid from the pericardial sac. The major goal is to prevent cardiac tamponade, which restricts normal heart action.
During
the procedure, the patient is monitored by ECG and hemodynamic pressure
measurements. Emergency resuscitative equipment should be readily available.
The head of the bed is el-evated to 45 to 60 degrees, placing the heart in
proximity to the chest wall so that the needle can be inserted into the
pericardial sac more easily. If a peripheral intravenous device is not already
in place, one is inserted, and a slow intravenous infusion is started in case
it becomes necessary to administer emergency medications or blood products.
The
pericardial aspiration needle is attached to a 50-mL sy-ringe by a three-way
stopcock. Several possible sites are used for pericardial aspiration. The
needle may be inserted in the angle be-tween the left costal margin and the
xiphoid, near the cardiac apex; at the fifth or sixth intercostal space at the
left sternal mar-gin; or on the right sternal margin of the fourth intercostal
space. The needle is advanced slowly until it has entered the epicardium and
fluid is obtained. The ECG can help determine when the needle has contacted the
epicardium. The cable of a precordial lead is attached to the aspirating needle
with alligator clamps; con-tact with the epicardium is seen by ST segment
elevation on the ECG. During the procedure, drainage fluid must be checked for
clotting. Although not entirely accurate, the guideline is that peri-cardial
blood does not clot readily, whereas blood obtained from inadvertent puncture
of one of the heart chambers does clot.
A
resulting fall in central venous pressure and an associated rise in blood
pressure after withdrawal of pericardial fluid indi-cate that the cardiac
tamponade has been relieved. The patient almost always feels immediate relief.
If there is a substantial amount of pericardial fluid, a small catheter may be
left in place to drain recurrent accumulation of blood or fluid. Pericardial
fluid is sent to the laboratory for examination for tumor cells, bacterial
culture, chemical and serologic analysis, and differential blood cell count.
Complications
of pericardiocentesis include ventricular or coronary artery puncture, dysrhythmias,
pleural laceration, gas-tric puncture, and myocardial trauma. After
pericardiocentesis, the patient’s heart rhythm, blood pressure, venous
pressure, and heart sounds are monitored to detect any possible recurrence of
cardiac tamponade. If it recurs, repeated aspiration is necessary. Cardiac
tamponade may require treatment by open pericardial drainage (pericardiotomy).
The patient is ideally in an intensive care unit.
PERICARDIOTOMY
Recurrent
pericardial effusions, usually associated with neoplastic diseases, may be
treated by a pericardiotomy
(pericardial window). The patient receives a general anesthetic, but
cardiopulmonary bypass is seldom necessary. A portion of the pericardium is
ex-cised to permit the pericardial fluid to drain into the lymphatic system.
Uncommonly, catheters are placed between the peri-cardium and abdominal cavity
to drain the pericardial fluid. The nursing care is the same as that described
for other cardiac surgery .
Related Topics