Chapter: Paediatrics: Practical procedures
Paediatrics: Umbilical arterial catheter
Umbilical arterial catheter
An umbilical arterial catheter
(UAC) can be used in newborns up to 48hr old for invasive BP monitoring,
continuous blood gas monitoring, blood sampling, fluid infusion, and/or
exchange transfusion.
Site
To avoid the origins of the
coeliac, mesenteric, and renal arteries, the tip of the catheter should be
positioned in the aorta above the diaphragm at the T8–T10 vertebral level or in
the distal aorta at the L3–L4 level.
Equipment
•
Antiseptic
solution, e.g. 0.5% chlorhexidine.
•
Sterile
surgical instruments including fine forceps, blunt-ended dilator probe,
scalpel, artery forceps, scissors, suture forceps, sutures.
•
Sterile
drapes, gown, gauze swabs, and gloves.
•
Umbilical catheters: 3.5Fr if birth weight <1500g;
5.0Fr for newborns 1500g. Catheters
with a terminal electrode can be used for continuous measurement of arterial O2
and CO2 concentrations.
•
3-way
taps, IV extension sets, syringes, cord ligature.
•
5–10mL
syringes, one containing heparinized saline (1Ut/mL).
•
BP
transducer if monitoring is intended.
Procedure
•
Monitor
baby closely during procedure, e.g. O2 saturation monitoring.
•
An
assistant should hold the baby’s legs down with the infant supine.
•
Calculate
the distance (cm) to insert the catheter from the umbilicus to the aorta at T8–10 level using the formula:
•
Insertion
distance = 3 × weight (kg) + 9 + umbilicus stump
length.
• To control bleeding, tie a cord
ligature around the umbilicus stump.
•
Catheter
insertion should be performed using strict aseptic technique.
•
Wash
hands and put on sterile gloves, gown, +/– surgical mask.
•
Connect
a 3-way tap to catheter and prime with heparinized 0.9% saline (do not use
heparinized saline if coagulation testing is required).
•
Clean
cord and periumbilical area with antiseptic solution.
•
Surround
periumbilical area with sterile towels to create sterile field.
•
Clamp
the umbilical cord horizontally with artery forceps 0.5–1cm above umbilical
skin. Using the artery forceps as a guide, cut the umbilical cord horizontally and
immediately below with the scalpel.
•
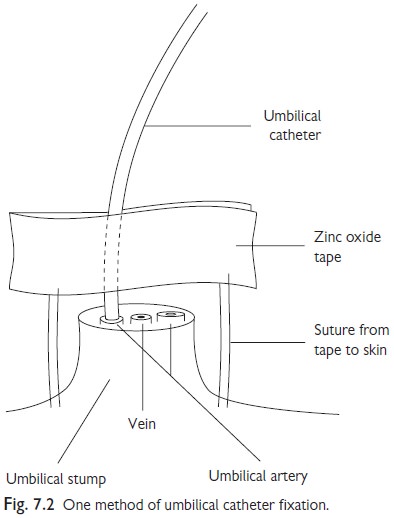
Identify
the two umbilical arteries and umbilical vein (see Fig. 7.2).
•
Dilate
the end of one of the arteries with fine forceps or a probe until wide enough
for the catheter tip to be easily introduced.
•
Gently
advance catheter the calculated distance (see formula). If resistance is met
put gentle traction on the umbilicus using artery forceps as this often eases
insertion down the spiral umbilical artery.
•
Aspirate
blood to confirm position and take required samples. Note: arterial blood should pulsate and still bleed if catheter hub
is held above infant (unlike blood from the umbilical vein).
•
Secure
catheter by fixing a zinc oxide flag around the catheter and then suture it to
the stump (see Fig. 7.2). Ligate remaining vessels with a separate purse string
suture. Remove cord ligature and check for bleeding.
•
Connect
catheter to 3-way tap and IV infusion set. BP monitoring can be performed by
connecting appropriate pressure transducer.
•
Confirm
correct placement with a combined CXR/AXR. Catheter should loop initially
downwards to the pelvis as it traverses the iliac arteries before ascending up
the aorta.
•
Check
perfusion of the perineum and lower limbs. If ischaemia occurs, this usually
may be corrected by an IV bolus of 0.9% saline or albumin. If ischaemia
remains, remove the catheter immediately.
•
Following
insertion, the abdomen should remain exposed to allow immediate observation of
any haemorrhage, e.g. from accidental removal of catheter.
As soon as the catheter is no
longer required, it should be removed. Cut the surrounding suture, then slowly
withdraw it, taking several minutes to remove the final few centimetres from
the artery. Then apply pressure or suture to limit any bleeding.
Related Topics